
![]()

![]()

![]()
![]()
 Page
Page
1 Introduction
1.1 Background
1.2 Purpose of HILs
1.3 Interpretation and use of the HILs
1.3.1 Limitations on the use of the HILs
1.3.2 What does ‘exceedence’ of an HIL mean?
1.4 Principles and methodology for generating the HILs
1.5 Objectives
2 Presentation of the health-based investigation levels
2.1 Stockholm Convention
2.2 Summary of HILs
2.2.1 Laboratory level of reporting
2.2.2 Polycyclic aromatic hydrocarbons
2.2.3 Toxicity surrogate approach
2.2.4 Inorganic mercury
2.2.5 PCBs
2.2.6 Interim HILs for volatile organic chlorinated compounds
2.2.7 Free cyanide
2.2.8 Home-grown produce
3 Generic land use scenarios
3.1 Introduction
3.2 Description of the generic land use scenarios
3.2.1 HIL A values – residential land use scenario with garden/accessible soil
3.2.2 HIL B values residential scenario with minimal opportunities for soil access
3.2.3 HIL C values public open space scenario
3.2.4 HIL D values - commercial/ industrial scenario
3.2.5 Sensitive populations
3.3 Exposure pathways
3.4 Application of the HILs to alternative land use scenarios
4 Toxicity assessment
4.1 Sources of toxicity data
4.2 Approach for carcinogenic contaminants
4.3 Toxicity approach for dermal exposure
4.4 Background exposure and contribution of soil to total exposure
4.5 Bioavailability and bioaccessibility
4.6 Speciation
4.7 Toxicity of groups of substances
5 Exposure assessment
5.1 Exposure pathways
5.2 General human characteristics applied in the derivation of the HILs
5.2.1 Body weight
5.2.2 Exposure duration and frequency
5.2.3 Averaging time
5.3 Pathway-specific exposure assumptions
5.3.1 Incidental ingestion of surface soil and dust
5.3.2 Dermal contact with surface soil and dust particulates
5.3.3 Indoor and outdoor inhalation of dust
5.3.4 Indoor and outdoor inhalation of vapours derived from soil
5.3.5 Consumption of home-grown produce
5.4 Blood lead modelling
5.4.1 Modelling adult exposures to lead
5.4.2 Modelling child exposures to lead
5.4.3 Bioavailability and bioaccessibility of lead
5.5 Vapour assessment
5.5.1 Introduction
5.5.2 Indoor exposures
5.5.3 Outdoor exposures
6 Risk characterisation how the HILs were generated
6.1 Risk characterisation and calculation of HILs
6.2 Target risk levels
6.3 Presentation of HILs
6.4 Uncertainty and sensitivity analysis
6.4.1 HIL uncertainty analysis
6.5 HIL sensitivity analysis
6.5.1 Soil fraction of organic carbon
6.5.2 Vapour intrusion rate
7 Bibliography
8 Glossary
9 Shortened forms
Appendix A Derivation of HILs and interim HILs
Appendix B Equations for derivation of HILs and interim HILs
Appendix C Calculations for HILs and interim HILs for generic land uses
Appendix D Blood lead model assumptions
This document presents the health investigation levels (HILs) for soil and describes their derivation. Schedules B7a and B7b to the National Environment Protection (Assessment of Site Contamination) Measure 1999 (the NEPM) have been updated and combined in this revised Schedule B7.
A review of the NEPM (NEPC 1999) was carried out during 20052006 at the request of the National Environment Protection Council (NEPC). The review recommended changes to improve the effectiveness and efficiency of the NEPM by addressing technical, scientific and health risk issues raised by site assessors, consultants, land developers, auditors and the public (NEPC 2006).
The recommendations from the NEPM review that relate to the HILs are as follows:
The requirement for additional HILs was also discussed at the 5th National Workshop on the Assessment of Site Contamination (NEPC 2003), at which some new HILs were proposed, and a list of possible candidate substances was produced.
This revised Schedule B7 addresses the findings of the NEPM review process. It presents an expanded list of HILs in accordance with the above recommendations, and sets out the revised and updated methodology adopted to derive the HILs. The methodology presented here is also applicable to site-specific health risk assessment. Further guidance on site-specific health risk assessment is provided in Schedule B4 Guideline on site-specific health risk assessment methodology.
The HILs (including interim HILs) are scientific, risk-based guidance levels (or Tier 1 criteria) designed to be used in the first stage of an assessment of potential risks to human health from chronic exposure to contaminants. The HILs are referred to by regulators, auditors and consultants in the initial process of assessing site soil contamination.
HILs are defined as the concentration of a contaminant above which further appropriate investigation and evaluation will be required.
Levels in excess of the HILs do not imply unacceptability or that a significant health risk is likely to be present. Similarly, levels below the HILs do not necessarily imply acceptability or that a health risk is not likely to be present, particularly if more sensitive populations[1] are present or the assumptions for land use scenarios are not appropriate.
The HILs are designed to be used to define the contaminants that require a more detailed (Tier 2) risk assessment. The tiered process of health risk assessment into which the HILs fit is described in detail in Schedule B4.
The HILs have been designed to be protective of the health of most people who could potentially be exposed to soil contaminants under four broad land use categories. For people within sensitive populations; for example, the immunosuppressed, those with pre-existing illness, or those with pica behaviour, the HILs may not be sufficiently protective of health. These issues would need to be addressed in a site-specific assessment.
The HILs have been developed under four broad land use categories (discussed in detail in Section 3). To estimate potential human exposure to soil contaminants within each of these land use categories, generic assumptions have been made about the environment, human behaviour, the physicochemical characteristics of contaminants, and the fate and transport of contaminants in soil (refer to Sections 3 and 4). The HILs have been derived by comparing estimated exposures with toxicity criteria using a quantitative modelling process. The toxicity criteria for all of the contaminants addressed in this guidance are outlined in the toxicity profiles included in Appendix A.
As indicated above, the HILs are not intended to be used as clean-up levels for contaminated sites. The decision on whether clean-up is required and, if so, to what extent, should be based on site-specific assessment and risk management options. Health risk assessment is one aspect of making the decision, with other considerations such as practicality, timescale, effectiveness and cost also being important.
The information in this Schedule is designed to assist risk assessors in the application of HILs to assess the potential risks posed to human health by soil contaminants, in a preliminary site assessment. Critical to this judgement is whether the conceptual site model (CSM) used to describe any of the generic land use categories is representative of the site in question.
The CSM for some sites may identify other potential risks from site contamination that are not covered by the HILs, including:
The potential for soil contaminant concentrations to vary significantly over a site means that a representative number of samples are required for an adequate understanding of the site. Recommendations regarding the sampling requirements for contaminated sites are described in Schedule B2.
Subject to the condition that site users are not identified as belonging to sensitive sub-populations, a site may be considered suitable for an intended land use provided that contaminant concentrations are less than the relevant HILs, with evidence from a sufficient number of samples and a spatially representative sampling design. In a situation where contaminant concentrations in some samples at a site exceed the HILs, statistical analysis may assist in the description and assessment of soil data in relation to the HILs.
HILs should only be used where there has been adequate characterisation of a site (that is, appropriate representative sampling has been carried out).
As a minimum, the maximum or 95% UCL should be compared to the HILs. However, where there is sufficient data and it is appropriate for the exposure being evaluated, the arithmetic mean (or geometric mean in the case of a log normal distribution) should also be compared to the HILs. The relevance of localised elevated values should be considered and should not be obscured by consideration only of the relevant mean of the results. The results should meet the following criteria:
However no single summary statistic will fully characterise a site and appropriate consideration of relevant statistical measurements should be used in the data evaluation process and iterative development of the CSM (refer to Schedule B2, Section 4). The preferred approach is to examine a range of summary statistics including the contaminant range, median, arithmetic/geometric mean, standard deviation and 95% UCL. Further information is provided in Section 11 of Schedule B2.
The application of interim HILs also needs to take into consideration soil vapour data. This data should be evaluated in order for it to be used in the appropriate exposure scenario at a site. The relevance of conducting statistical tests (other than the arithmetic mean) should be evaluated for soil vapour data. Where data is limited or it is not relevant (for the purpose of assessing exposure) to conduct statistical analysis, the maximum soil vapour concentration can be compared against the interim HIL.
Exceedence of the HILs does not automatically imply that quantitative modelling at Tier 2 risk assessment stage is warranted. Similarly, concentrations less than that of the HILs do not necessarily imply that a Tier 2 risk assessment stage is not warranted. As already mentioned, HILs are not intended to indicate a clear demarcation between ‘acceptable’ and ‘unacceptable’ soil contaminant levels.
The decision to proceed or not to proceed with additional data collection and risk assessment should always be considered with reference to the site-specific exposure pathways, the consequences of exposure, and the characteristics of the exposed population (i.e. site-users).
The derivation of HILs follows the same five-step process central to Australian risk assessment practice as outlined in Schedule B4 and enHealth (2012a).
Fundamentally, the HILs have been derived as scientifically-based, generic criteria designed to be used in the first stage of an assessment of potential risks to human health from chronic exposures to contaminants. The underlying principles/considerations adopted in deriving the HILs are as follows:
This Schedule is structured according to the five-step risk assessment process (also refer to Appendices A to D for more specific detail), which is summarised below.
The HIL values are the outcomes of this risk assessment process and are presented in Tables 2 and 3 in this Schedule.
The scope and purpose for the derivation of the HILs was established during the NEPM review described in Section 1.1. The key objectives are:
This chapter presents the HILs for soil contaminants. The HILs have been designed to be protective of the health of most people who could potentially be exposed to soil contaminants under four broad land use categories, not including sensitive sub-populations:
Further details of each of these generic land use scenarios are provided in Section 3 of this Schedule. Note that HIL A is applicable to homes with a garden large enough to provide an area where children could play and/or where vegetables could be grown. A small paved back yard with small flower beds but without a lawn would be included in HIL B.
The terms ‘low’, ‘medium’ and ‘high’ density are commonly used in land use zonings in Australia. Low density would normally be equivalent to HIL A and high density to HIL B. The definition of medium density however is not consistent and the relevance of HIL A or HIL B to this land use should be considered on a site-specific basis.
The Stockholm Convention on POPs is a global convention to protect human health and the environment from chemicals that persist in the environment for long periods, become widely distributed geographically and accumulate in the fatty tissue of humans, domesticated food animals and wildlife. Exposure to POPs can lead to serious health effects including certain cancers, birth defects, dysfunctional immune and reproductive systems, greater susceptibility to disease, and even diminished intelligence.
The Stockholm Convention requires its parties to take measures to eliminate or reduce the release of POPs into the environment. This convention was adopted in 2001 and came into force in 2004. Australia ratified the convention in 2004.
The POPs included in the Stockholm Convention are covered by three separate annexes:
Under the terms of the Stockholm Convention, a regular review process allows for additional chemicals to be nominated, and after appropriate review, included in the Convention.
Chemicals added to the Convention in 2009 included:
Further consideration of the data available for these chemicals and the potential for developing an HIL will be included in subsequent reviews of the HILs.
HILs have been developed for all POPs adopted in the Stockholm Convention prior to 2009, with the exception of PCDD/PCDF. These chemicals do not have HILs but a contaminated site that has a history suggesting the likely presence of dioxins would require a site-specific health risk assessment (refer Section 12 of Schedule B2).
The HIL values for the four broad land use categories are presented in Table 2. Additional information to assist in the use of the HIL values during a site-specific assessment is presented below.
The available laboratory detection limits should be reviewed in conjunction with the HILs to ensure that the most relevant detection limit is employed and the collection of additional site-specific information (for example, soil vapour data) is appropriate.
The assessment of the health risk posed by polycyclic aromatic hydrocarbons (PAHs) is complicated by the large number of individual PAHs and the complex mixtures that exist in the environment. A specific HIL value has only been derived for the carcinogenic PAHs, based on the toxicity of benzo(a)pyrene (BaP). For other carcinogenic PAH compounds or carcinogenic PAH mixtures, the toxicity equivalence factor (TEF) approach is recommended. The TEF approach assumes that the risk posed by individual carcinogenic PAHs is additive and proportional to the potency of each compound in the mixture. The potency of individual carcinogenic PAHs is expressed relative to benzo(a)pyrene.
Naphthalene, the most significant volatile PAH, requires separate assessment, as the vapour inhalation pathway is of greater significance. The assessment of potential naphthalene exposures should consider the Health Screening Level (HSL) for naphthalene derived from exposure to petroleum hydrocarbons (Schedule B1).
To apply the HIL to a mixture of carcinogenic PAHs, the concentration of each carcinogenic PAH in the mixture should be multiplied by the respective TEF outlined in Table 1 and the resulting values summed for comparison with the benzo(a)pyrene HIL value.
Table 1. Toxicity equivalence factors for PAHs
PAH | TEF |
Benzo(a)anthracene | 0.1 |
Benzo(a)pyrene | 1 |
Benzo(b+j)fluoranthene | 0.1 |
Benzo(g,h,i)perylene | 0.01 |
Benzo(k)fluoranthene | 0.1 |
Chrysene | 0.01 |
Dibenz(a,h)anthracene | 1 |
Indeno(1,2,3-cd)pyrene | 0.1 |
Source: CCME (2008) | |
A number of groups of chemicals addressed in the derivation of the HILs contain a number of similar chemical constituents where there is a mix of information on individual chemicals. In cases where there is insufficient information to derive separate HILs for each individual compound, the toxicity surrogate approach has been applied to the derivation of HILs for these substances. This approach involves the generation of an HIL value for a single ‘indicator’ chemical and the application of this information directly to the assessment of other similar chemicals within the group.
HIL values derived using the toxicity surrogate approach include cresols (methylphenols), DDT, aldrin and dieldrin, polychlorinated biphenyls (PCBs) and polybrominated diphenyl ethers (PBDEs). The sum of all the individual chemical concentrations within each of these groups can be compared directly to the HIL value, based on the assumption that their effects are similar and additive.
The HIL value for inorganic mercury was derived using the physicochemical characteristics of mercuric mercury (Hg2+). This value does not include the potential for the inhalation of vapours derived from elemental mercury. A site-specific assessment should be undertaken if elemental mercury is present or suspected to be present.
The HIL value for PCBs relates to non-dioxin-like PCBs only. Where the assessment indicates the potential for a PCB source to be present on the site, the HILs may not be sufficiently protective. Hence a site-specific assessment of exposure to all PCBs, including dioxin-like PCBs should be undertaken.
Investigation levels derived for the volatile organic chlorinated hydrocarbons (VOCCs) are presented as interim HILs, as the methodology adopted in the derivation of these values is not as fully developed as that for the non-volatile HILs. The application and revision of these values will rely on improvements in the understanding of the behaviour of chlorinated solvents in transferring from soil to indoor air.
The interim HIL values derived for volatile compounds are driven by the vapour intrusion pathway (that contributes >99% of the total risk where all pathways are considered). However, it is noted that there are limitations and uncertainties associated with the assessment of volatile contaminants on the basis of soil concentrations. As these limitations are significant for volatile organic chlorinated compounds, interim HILs for soil have not been derived. Rather it is recognised that where indoor/ambient air data cannot be collected (or the data is affected by background sources), the most relevant approach to the assessment of this pathway is through the collection of soil vapour data. On this basis, interim HILs have been developed for soil vapour.
It is noted that for short-duration exposures such as during intrusive works where direct contact with the source may occur (not addressed in the derivation of HILs) other exposure pathways (in addition to vapour inhalation) may be more significant and require evaluation on a site-specific basis.
Interim HILs are relevant to soil vapour that may have been derived from a soil or groundwater source, or a combination of both.
The values have been derived assuming a slab-on-ground building is present directly above the contaminant source. Groundwater, if present, is assumed to be deeper than the building foundations (i.e. no contact between the building foundations and groundwater at any time).
In circumstances where the building type differs (for example, inclusion of a crawl space or basement), or where there is the potential for preferential vapour pathways to be present, a site-specific assessment should be undertaken.
Further information on the assessment of volatile substances, including VOCCs, can be found in Schedule B2.
Cyanide-impacted soils are often dominated by stable cyanide-metal complexes that are of low inherent toxicity and are non-volatile. No HIL for complexed cyanide is presented because of the low toxicity. Free cyanide (defined as the cyanide ion (CN-) or hydrogen cyanide (HCN)) is only formed in environments that are dominated by weak cyanidemetal complexes (for example, silver cyanide) and dissolved cyanide complexes.
The HIL has been derived on the basis of free cyanide and it is recognised that the measurement of free cyanide in soil is difficult. Measurement is difficult due to instability of not only free cyanide but also cyanide metal complexes that can produce free cyanide. A cautious approach (Department of Resources, Energy and Tourism 2008; ICMI 2009), is to measure free cyanide and other dissociable cyanide species that could produce free cyanide either by dilution or by other natural processes (refer to US EPA method 9016). The US EPA Weak Acid Dissociable Cyanide (WAD) method measures free cyanide plus the cyanide associated with most unstable metal cyanide complexes. The WAD cyanide refers to any species where cyanide is liberated at pH 4.5. Such species include HCN (aq) and CN-, and the majority of Cu, Cd, Ni, Zn and Ag complexes. If the WAD result conforms to the HIL, then the free cyanide level is also in compliance with the HIL.
The presence of free cyanide in soil and the potential for formation of HCN is complex and depends on the soil pH, ionic strength and complexation. The ability of standard vapour models to estimate the concentration of HCN in air (indoors and outdoors) is considered to be poor (RIVM 2001) due to the complexity of the processes involved. Hence, the HIL derived for free cyanide does not address issues that may be associated with the formation of HCN gas and potential exposures indoors and outdoors. These exposures need to be addressed on a site-specific basis.
Where relevant for each compound assessed, the HIL A values assume that 10% of vegetable and fruit consumption comes from produce grown on the contaminated site. Details on the potential significance of uptake into home-grown fruit and vegetable crops are presented in the chemical summaries in Appendix A.
Intakes from other home-grown produce, namely eggs and poultry meat, have not been addressed in the derivation of the HILs. These intakes/exposures may be a significant exposure pathway for some soil contaminants and should be assessed on a case-by-case basis.
Table 2. Health investigation levels for soil contaminants
Chemical | Health-based investigation levels (mg/kg) | |||
Residential1 A | Residential1 B | Recreational1 C | Commercial/ | |
Metals and Inorganics | ||||
Arsenic2 | 100 | 500 | 300 | 3000 |
Beryllium | 60 | 90 | 90 | 500 |
Boron | 4500 | 40 000 | 20 000 | 300 000 |
Cadmium | 20 | 150 | 90 | 900 |
Chromium (VI) | 100 | 500 | 300 | 3600 |
Cobalt | 100 | 600 | 300 | 4 000 |
Copper | 6000 | 30 000 | 17 000 | 240 000 |
Lead3 | 300 | 1200 | 600 | 1500 |
Manganese | 3800 | 14 000 | 19 000 | 60 000 |
Mercury (inorganic)5 | 40 | 120 | 80 | 730 |
Methyl mercury4 | 10 | 30 | 13 | 180 |
Nickel | 400 | 1200 | 1200 | 6000 |
Selenium | 200 | 1400 | 700 | 10 000 |
Zinc | 7400 | 60 000 | 30 000 | 400 000 |
Cyanide (free) | 250 | 300 | 240 | 1500 |
Polycyclic Aromatic Hydrocarbons (PAHs) | ||||
Carcinogenic PAHs (as BaP TEQ)6 | 3 | 4 | 3 | 40 |
Total PAHs7 | 300 | 400 | 300 | 4000 |
Phenols | ||||
Phenol | 3000 | 45 000 | 40 000 | 240 000 |
Pentachlorophenol | 100 | 130 | 120 | 660 |
Cresols | 400 | 4700 | 4 000 | 25 000 |
Organochlorine Pesticides | ||||
DDT+DDE+DDD | 240 | 600 | 400 | 3600 |
Aldrin and dieldrin | 6 | 10 | 10 | 45 |
Chlordane | 50 | 90 | 70 | 530 |
Endosulfan | 270 | 400 | 340 | 2000 |
Endrin | 10 | 20 | 20 | 100 |
Heptachlor | 6 | 10 | 10 | 50 |
HCB | 10 | 15 | 10 | 80 |
Methoxychlor | 300 | 500 | 400 | 2500 |
Mirex | 10 | 20 | 20 | 100 |
Toxaphene | 20 | 30 | 30 | 160 |
Herbicides | ||||
2,4,5-T | 600 | 900 | 800 | 5000 |
2,4-D | 900 | 1600 | 1300 | 9000 |
MCPA | 600 | 900 | 800 | 5000 |
MCPB | 600 | 900 | 800 | 5000 |
Mecoprop | 600 | 900 | 800 | 5000 |
Picloram | 4500 | 6600 | 5700 | 35 000 |
Other Pesticides | ||||
Atrazine | 320 | 470 | 400 | 2500 |
Chlorpyrifos | 160 | 340 | 250 | 2000 |
Bifenthrin | 600 | 840 | 730 | 4500 |
Other Organics | ||||
PCBs8 | 1 | 1 | 1 | 7 |
PBDE Flame Retardants (Br1-Br9) | 1 | 2 | 2 | 10 |
Notes:
(1) Generic land uses are described in detail in Section 3.
HIL A: Residential with garden/accessible soil (home-grown produce <10% fruit and vegetable intake (no poultry)), also includes childcare centres, preschools and primary schools
HIL B: Residential with minimal opportunities for soil access; includes dwellings with fully and permanently paved yard space such as high-rise buildings and apartments
HIL C: Public open space such as parks, playgrounds, playing fields (e.g. ovals), secondary schools and footpaths. This does not include areas of undeveloped open space where the potential for exposure is lower and where a site-specific assessment may be more appropriate.
HIL D: Commercial/industrial includes premises such as shops, offices, factories and industrial sites.
(2) Arsenic: HIL for arsenic assumes 70% oral bioavailability. Site-specific bioavailability may be important and should be considered where appropriate (refer Schedule B7).
(3) Lead: HIL for lead is based on blood lead models (IEUBK for HILs A, B and C and adult lead model for HIL D) where 50% oral bioavailability has been considered. Site-specific bioavailability may be important and should be considered where appropriate.
(4) Methyl mercury: assessment of methyl mercury should only occur where there is evidence of its potential source. It may be associated with inorganic mercury and anaerobic microorganism activity in aquatic environments. In addition, the reliability and quality of sampling/analysis should be considered.
(5) Elemental mercury: HIL does not address elemental mercury. A site-specific assessment should be considered if elemental mercury is present, or suspected to be present.
(6) Carcinogenic PAHs: HIL for carcinogenic PAHs is based on the 8 carcinogenic PAHs and their respective TEFs (potency relative to BaP) adopted by CCME 2008. The BaP TEQ is calculated by multiplying the concentration of each carcinogenic PAH in the sample by its BaP TEF, given below, and summing these products.
PAH species | TEF | PAH species | TEF |
Benzo(a)anthracene | 0.1 | Benzo(g,h,i)perylene | 0.01 |
Benzo(a)pyrene | 1 | Chrysene | 0.01 |
Benzo(b+j)fluoranthene | 0.1 | Dibenz(a,h)anthracene | 1 |
Benzo(k)fluoranthene | 0.1 | Indeno(1,2,3-c,d)pyrene | 0.1 |
Where the BaP occurs in bitumen fragments it is relatively immobile and does not represent a significant health risk.
(7) Total PAHs: HIL for total PAH is based on the sum of the 16 PAHs most commonly reported for contaminated sites (WHO 1998). The application of the total PAH HIL should consider the presence of carcinogenic PAHs and naphthalene (the most volatile PAH). Carcinogenic PAHs reported in the total PAHs should meet the BaP TEQ HIL. Naphthalene reported in the total PAHs should meet the relevant HSL.
(8) PCBs: HIL for PCBs relates to non-dioxin-like PCBs only. Where a PCB source is known, or suspected, to be present at a site a site-specific assessment of exposure to all PCBs (including dioxin-like PCBs) should be undertaken.
Table 3. Interim soil vapour health investigation levels for volatile organic chlorinated compounds
Chemical | Interim soil vapour HIL (mg/m3) | |||
Residential1 A | Residential1 B | Recreational1 C | Commercial/ Industrial1 D | |
TCE | 0.02 | 0.02 | 0.4 | 0.08 |
1,1,1-TCA | 60 | 60 | 1200 | 230 |
PCE | 2 | 2 | 40 | 8 |
cis-1,2-dichloroethene | 0.08 | 0.08 | 2 | 0.3 |
Vinyl chloride | 0.03 | 0.03 | 0.5 | 0.1 |
Notes:
(1) Land use settings are equivalent to those described in Table 2 Footnote 1 and Section 3 of this Schedule, except for secondary school buildings which should be assessed against residential ‘A/B” for vapour intrusion purposes.
(2) Interim HILs for VOCCs are conservative soil vapour concentrations that can be adopted for the purpose of screening sites where further investigation is required on a site-specific basis. They are based on the potential for vapour intrusion indoors using an indoor air-to-soil vapour attenuation factor of 0.1 (for interim HIL A, B and D) and an outdoor air attenuation factor of 0.05 (interim HIL C).
(3) Application of the interim HILs is based on a measurement of shallow (to 1 m depth) soil vapour (or deeper where the values are to be applied to a future building with a basement) or sub-slab soil vapour.
(4) The applicability of the interim HILs needs to be further considered when used for other building types such as homes with a crawl-space and no slab which require site-specific assessment.
(5) Use of the interim HILs requires comparison with data that has been collected using appropriate methods and meets appropriate data quality requirements.
(6) Oral and dermal exposure should be considered on a site-specific basis where direct contact exposure is likely to occur.
Assessments of potential risks to human health resulting from site contamination are based on CSMs that identify the conditions through which exposure to contaminants can occur. The key components of a CSM are the contaminant source, receptors (human populations) and exposure pathways. For further information on developing CSMs refer to Schedule B2.
The source addressed in this Schedule is a soil source and this is the source represented in all CSMs presented. The HILs are not derived for the purpose of assessing groundwater sources. However the interim soil vapour HILs for VOCCs may be applied to soil vapour derived from a soil or groundwater source, or a combination of both for these compounds.
Four generic land use scenarios have been used to derive the HILs. These are based on the typical settings in Australia under which people may be exposed to contaminated soil. A separate set of HILs has been developed for each generic land use category, because the sensitive populations and intensity, frequency and means of exposure to soil contaminants can differ according to land use.
The four generic land use scenarios used in the derivation of the HILs are described below. Also in this Schedule is a description of the environment and buildings considered under each land use scenario, a description of the characteristics of relevant human populations, and relevant exposure pathways applied under each land use scenario. This information is designed to allow risk assessors to gauge the applicability of the HILs to the circumstances at individual sites. The assessment of soil contamination at sites that are not adequately represented by any of the standard land use scenarios is also discussed in this Schedule.
The generic land use scenarios considered in the development of the HILs are:
The HILs have been derived for the above land use scenarios based on long-term exposures for the most sensitive receptor populations exposed. The HILs are therefore considered to be protective of exposures to other receptor populations; however, the HILs do not specifically address short-duration exposures that may occur during construction and maintenance of a site (including intrusive works). These exposures should be addressed on a site-specific basis.
These land use scenarios are broadly consistent with exposure settings A, D, E and F respectively, as described in NEPC (1999). When land is used for more than one purpose, the HILs that are relevant to the more sensitive land use should be adopted for that site.
Residential land use includes a variety of building densities, ranging from separate low-density dwellings to high-density unit blocks. The residential land use scenario considered in the derivation of the HIL A values is low-density residential, including a sizeable garden (referring to the presence of sufficiently large areas of soil in a garden that may be accessible on a daily basis by young children and adults).
The HIL A values are also applicable to the preliminary assessment of potential risks at sites where children are likely to be the most sensitive human receptors, including childcare centres, kindergartens, preschools and primary schools and their integral playgrounds. The scenario is designed to represent a typical residential land use. The HIL A values will also be protective of circumstances where less exposure to soil would be likely (for example, older people, or without fruit and vegetable gardens).
It is noted that for people within sensitive sub-populations; for example, the immunosuppressed, those with pre-existing illness, or those with pica behaviour, the HILs may not be sufficiently protective of health and site-specific risk assessment (or criteria) or management strategies may be required.
This land use scenario assumes typical residential properties, consisting of single storey dwellings supported by ground-level slabs or multistorey dwellings where living areas are on the ground floor and there is accessible soil in the front and backyard areas.
These residences may have private gardens, consisting of lawns, garden beds and small vegetable gardens and areas of fruit trees, but no poultry. The occupants of the dwellings include adults, children and infants, who spend the majority of their time on the residential properties and use the outdoor areas of the residences on a frequent basis, for activities such as gardening or recreation. The CSM for this land use scenario is provided in Figure 1.
The derivation of soil HILs addresses all non-volatile compounds and exposure pathways. The interim soil vapour HILs for VOCCs address the vapour pathway, only for these compounds.

Figure 1. CSM for HIL A standard residential land use scenario with garden/accessible soil
The residential land use scenario considered for the HIL B values is high-density residential, not including a private garden. This land use scenario assumes typical residential unit blocks, consisting of multistorey buildings where living areas are on the ground floor (constructed on a ground level slab or above subsurface structures including basement car parks or storage areas).
Occupants of the buildings considered in the development of the HIL B values have access to yard spaces that are largely covered by permanent paving, with some small areas of landscaping or lawns. Opportunities for direct access to soil by residents of these buildings are therefore minimal but there may be some potential for residents to inhale, ingest or come into direct dermal contact with dust (particulates) derived from the soil on the site. Landscaped/playground (including sandpit) areas used for recreation within a high-density development should be assessed on the basis of the more conservative HIL C values.
The occupants of the dwellings are adults, children and infants who spend the majority of their time indoors within the residential properties, with some limited use of communal outdoor areas on site. The residents that are considered to be most susceptible to health risks associated with soil contaminants are the residents of ground floor units, due to the greatest potential for outdoor soil to be tracked indoors and vapour intrusion occurring with residences immediately overlying contaminated soil. The CSM for this land use scenario is provided in Figure 2.

Figure 2. CSM for HIL B residential land use scenario with minimal opportunities for soil access
It is noted that the derivation of soil HILs addresses all non-volatile compounds and exposure pathways. The interim soil vapour HILs for VOCCs address the vapour pathway only for these compounds.
Public open space land use includes a variety of exposure scenarios such as parks and playgrounds (including sandpits), recreational areas and playing fields that are fully accessible to the public and where the public may potentially spend a significant amount of time.
This land use scenario assumes that the open space areas are in areas where young children may have supervised access and use the area outside of the home environment for frequent short periods of time (up to 2 hours a day, 7 days a week). Other users may include older children and adults who may visit the area frequently for a range of recreational purposes. These open space areas may contain lawns, gardens, vegetated areas and walkways, with some limited areas of hardstand and some areas of exposed soil. The open space areas may contain buildings such as amenity blocks, but individuals who visit these areas are considered to spend the majority of their time outdoors where the exposure is limited to outdoor soil.
The CSM for this land use scenario is provided in Figure 3. In addition, the derivation of soil HILs addresses all non-volatile compounds and exposure pathways. The interim soil vapour HILs for VOCCs addresses the vapour pathway only for these compounds.
Scenario HIL C does not directly apply to non-recreational open spaces, such as road reserves, where the potential for exposure (and frequency of exposure) is lower and which should be subject to a site-specific assessment (where appropriate).

Figure 3. CSM for HIL C public open space land use scenario
The land use scenario considered for the HIL D values is commercial/industrial, which assumes typical commercial or light industrial properties, consisting of single or multistorey buildings where work areas are on the ground floor (constructed on a ground level slab) or above subsurface structures (such as basement car parks or storage areas).
The land use scenario does not include more sensitive uses that may be permitted under relevant commercial or industrial zonings. These more sensitive uses include childcare, educational facilities, caretaker residences and hotels and hostels, etc. Information on uses permitted under local council zoning schemes for commercial/industrial land use can be obtained from local council planning zones/schemes. Should these more sensitive uses be permitted, then HIL A or HIL B values should be considered.
The dominant users of commercial/industrial sites are adult employees, who are largely involved in office-based or light indoor industrial activities. The employees who are most susceptible to health risks associated with volatile soil contaminants are the employees who work in offices on the ground floor, as the greatest potential for vapour intrusion occurs with workspaces immediately overlying contaminated soil.
The outdoor areas of the commercial/industrial facilities are largely covered by hardstand, with some limited areas of landscaping or lawns and facilities. Employees may make use of outdoor areas of a commercial/industrial premises for activities such as meal breaks. Opportunities for direct access to soil by employees using these facilities are likely to be minimal, but there may be potential for employees to inhale, ingest or come into direct dermal contact with dust particulates derived from the soil on the site. The CSM for this land use scenario is provided in Figure 4.
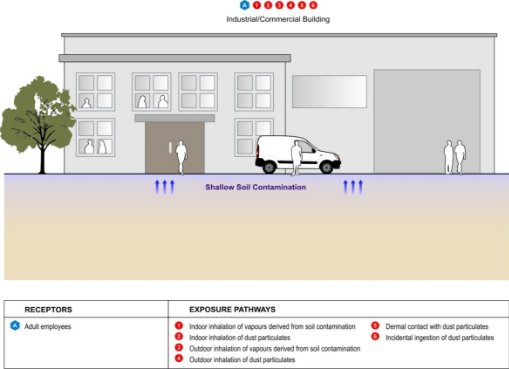
Figure 4. CSM for HIL D commercial/industrial land use scenario
The derivation of soil HILs addresses all non-volatile compounds and exposure pathways. The interim soil vapour HILs for VOCCs address the vapour pathway only for these compounds.
The HILs for each land use scenario have been developed to be protective of the majority of human populations that are sensitive to potential health risks from soil contamination. The HILs depend upon both the exposure scenario and the toxicity reference values selected for the contaminant.
The level of exposure of a given human population to health risks within a particular land use scenario is related to physiological factors (for example, children are often more heavily exposed to contaminants than adults because, in comparison to their body weight, they have higher rates of inhalation and ingestion and a larger skin surface area) and the frequency, extent and duration of exposure (for example, permanent residents are a more sensitive population than intermittent visitors).
The toxicity reference values were selected from collated peer-reviewed sources using the data sources described in Schedule B4.
Unless otherwise noted, all of these sources provide criteria that represent tolerable levels of exposure to the population inclusive of those individuals considered to be sensitive to the contaminant concerned. The toxicity criteria therefore inherently incorporate protection to sensitive populations. Different sources of toxicity criteria provide slightly differing approaches to protection of sensitive populations because they are derived by different bodies (for example, NHMRC, WHO and US EPA), which may have differing policy positions. The source and basis of selected toxicity reference values are presented on a compound-specific basis in Appendix A.
The populations that are usually most sensitive to health risks associated with soil contamination in both low-density and high-density residential settings and in the open space scenario are young children aged 23 years. The characteristics of exposed populations applied in the development of the HILs have been derived in accordance with the recommendations outlined by enHealth (2012a). Young child residents and recreational users, while assessed on the basis of parameters relevant to 23 year old children, have been taken to be representative of children aged between 0 and 6 years of age who live within the same dwelling or visit the same open space area for their entire childhood.
Adults of working age are the population usually most sensitive to health risks associated with soil contamination within the generic commercial/industrial land use scenario. Although many commercial premises welcome children on an intermittent basis, it is unlikely that children visit the majority of workplaces frequently. Similarly, in commercial premises where children are regular visitors, such as shopping centres, both the duration and frequency of child exposures are generally lower than that of a full-time adult employee.
In accordance with the recommendations outlined in enHealth (2004), the adult employees addressed in the HIL D values have been considered to work within the same commercial/industrial premises for their full working life (30 years). The HILs developed for the commercial/industrial land use scenario are not applicable to a site used frequently by more sensitive groups such as children (within childcare centres, hospitals and hotels) and the elderly (within hospitals, aged care facilities and hospices).
For each land use, consideration has been given to the ways in which people could be exposed to soil contamination. The term ‘exposure pathway’ is used to describe the course that a contaminant takes from its source area to reach an exposed population. An exposure pathway is considered to be complete when a receptor (for example, resident or worker) receives a dose of the contaminant.
For the purposes of developing the HILs, it has been assumed that exposure could potentially occur via the following exposure pathways:
Not all exposure pathways are relevant to all land use categories. For example, in the open space scenario, it is assumed that there are no permanently occupied buildings in which indoor air could be impacted by vapours derived from the underlying soil. Hence, exposure to soil contaminants within open space areas occurs largely in the outdoor environment and the exposure pathway of indoor vapour inhalation is not applicable. Similarly, the consumption of home-grown produce and soil adhering to home-grown produce is only applicable to the low-density residential land use scenario.
The exposure pathways considered in the development of HILs for each of the four different land use categories are summarised in Table 4.
Table 4. Exposure pathways considered for the four generic land use categories
Exposure pathways | Land use scenario | |||
| HIL A | HIL B | HIL C | HIL D |
Indoor inhalation of dust | | | Χ | |
Outdoor inhalation of dust | | | | |
Dermal contact with shallow soil and dust | | | | |
Incidental ingestion of shallow soil and dust | | | | |
Ingestion of home-grown vegetables and fruit | | Χ | Χ | Χ |
Ingestion of home-grown poultry and/or eggs | Χ | Χ | Χ | Χ |
Ingestion of soil adhering to home-grown produce | | Χ | Χ | Χ |
Indoor inhalation of vapours derived from soil | I | I | Χ | I |
Outdoor inhalation of vapours derived from soil | Χ | Χ | I | Χ |
indicates exposure pathway has been considered in the derivation of the HILs | ||||
I indicates exposure pathway has been considered in the derivation of the interim soil vapour HILs for VOCCs | ||||
Χ indicates that exposure pathway has not been considered in the derivation of the HILs or interim soil vapour HILs | ||||
The generic land use scenarios used in the development of the HILs will be unlikely to accurately reflect all of the conditions present at an individual site. As the HILs are intended to represent a ‘reasonable worst case’ for each land use, provided that the site land use is broadly equivalent to one of the HIL scenarios, the HILs will provide for a health protective Tier 1 screening assessment. There are some limitations to the use of HILs, as described previously.
For land uses not specifically referred to in the scenario descriptions, there are two options:
The methodology presented in this Schedule may be used to derive ‘HIL equivalent’ values applicable to site-specific circumstances, by amending appropriate exposure settings and site characteristics values.
The toxicity assessment component of the derivation of the HILs involved the review of the published toxicity reference values that have been developed by various published peer-reviewed government authorities and other agencies, and selection of the appropriate reference value for each of the soil contaminants.
For all contaminants considered in the derivation of HILs, toxicity reference values (TRVs) have been identified following review of relevant information from published peer reviewed sources. The term TRV has been adopted as a general term that is used to define the health-based toxicity value used to derive an HIL. TRVs include both threshold and non-threshold toxicity values.
For threshold chemicals, TRVs reflect a measure of tolerable daily exposure and include values that are presented by different agencies using a range of different terms. Most commonly these include an ADI (acceptable daily intake), TDI (tolerable daily intake), TC (tolerable concentration in air), RfD (reference dose), RfC (reference concentration), MRL (minimal risk level), and REL (reference exposure level).
For non-threshold chemicals, TRVs reflect a cancer risk value commonly referred to as a cancer slope factor (CSF) or unit risk (UR).
TRVs used in the derivation of HILs are presented in Appendix A. The approach that applies to the identification of all the TRVs used in the derivation of HILs is described herein. Where both threshold and non-threshold TRVs have been considered, both approaches have been considered; however, the HIL presented is the lowest value derived based on the more sensitive effect.
The TRVs used in the derivation of the HILs have been sourced from peer reviewed references using the data sources presented in Schedule B4.
For the purpose of deriving the HILs, chemicals that are classified by the International Agency on Research on Cancer (IARC) as Category 1, 2A or 2B carcinogens have been considered to be carcinogenic and those classified Category 3 and 4 have been considered non-carcinogenic. There are limitations with this assumption; however, Category 3 and 4 chemicals rarely have adequate data for assessment as carcinogens. There are a number of Category 2 chemicals that also lack adequate carcinogenic dose response data and have, therefore, been assessed using non-cancer toxicity criteria; this is highlighted in the toxicity summary where relevant.
Consistent with the approach outlined in Schedule B4, the approach adopted for the assessment of carcinogens has been determined based on the mode of action. For genotoxic carcinogens, a non-threshold approach has been adopted (where data is available); however, for carcinogens that are non-genotoxic, a threshold approach has been adopted.
Where specific dermal TRVs are available, these were used for the assessment of dermal contaminant toxicity; in their absence, oral TRVs have been used for the dermal hazard assessment. Oral TRVs almost invariably relate to applied dose rather than absorbed dose. Hence, where there is suitable chemical-specific data available, the TRV has been adjusted by a gastrointestinal absorption factor (GAF) to produce a reference value relating to absorbed dose (US EPA 2004b).
The equations applied in this adjustment (relevant on a chemical-specific basis) are outlined as follows:
Threshold TRVDermal = Threshold TRVOral x GAF
Non-threshold TRVDermal = Non-threshold TRVOral /GAF
where
TRVOral = oral toxicity reference value
TRVDermal = dermal toxicity reference value
GAF = gastrointestinal absorption factor.
Background levels of contamination are the chemical concentrations present in the environment as a result of everyday activities (for example, emissions from motor vehicles, industry or efflux from the ground surface in the case of volatiles) or natural sources (for example, dissolution of mineral deposits). Chemicals present in food, air, water and consumer products all contribute to the quantity of the chemical that a person might be exposed to on a daily basis. The exposure from non-site sources is referred to throughout this document as ‘background exposure’.
The threshold TRV is associated with a tolerable total intake from all sources, which includes food, air, water, consumer products and contamination sources. If it is known that a significant background exposure is likely to exist, then a proportion of the threshold TRV should be allocated to the background before comparing exposures derived from contamination in soil to the TRV.
This is only applied to threshold substances, because intakes of non-threshold contaminants are considered on the basis of an increase in risk, which is irrespective of background exposure (Health Canada 2004).
In the derivation of the HILs, this has been done on a chemical-specific basis by applying a factor to the threshold TRV, as outlined in the equations in Appendix B. Essentially this is calculated as follows for threshold contaminants:
TRV(adjusted) = (1 – Background) x TRV
The background concentration has been considered for each threshold chemical (refer to Appendix A) based on available data from Australia and, where limited data is available, from other countries. Where no data is available, an evaluation is undertaken on a chemical-specific basis with a default value for background exposure assumed where relevant.
It is possible for background exposure to be essentially negligible (contributing less than 5% of the threshold TRV) for chemicals that are not widely distributed in the environment. In these cases, 100% of the threshold TRV has been allocated to exposure from soil. This assumption should be considered further where site-specific conditions suggest otherwise.
In addition, it is also possible for background exposure to exceed the threshold TRV (for example, intakes of methyl mercury from fish), in which case, theoretically an HIL cannot be derived. A few approaches are available to address this problem. In the UK, when background exposure comprises greater than 50% of the threshold TRV, then the background exposure is taken to be 50% of the TRV (EA 2008). New Zealand guidance (MfE 2011b) has considered the proportion allocated to exposure from soil on a case-by-case basis. In the derivation of the HILs, a case-by-case approach has also been adopted.
Bioavailability and bioaccessibility are discussed and defined in Schedule B4.
Bioavailability (absolute) is the fraction or percentage of a compound which is ingested, inhaled or applied to the skin that actually is absorbed and reaches systemic circulation.
Relative bioavailability refers to the comparative bioavailability of different forms of a chemical or to different exposure media containing the chemical and is expressed as a fractional relative absorption factor.
Bioaccessibility is the fraction of a contaminant in an exposure medium that is soluble in the relevant physiological milieu (usually the gastrointestinal tract) and available for absorption.
Not all texts make an equivalent distinction between bioavailability (absolute and relative) and bioaccessibility, but in the assessment of contaminated soils it is a useful concept because it provides clarity on the modelling approach adopted in the derivation of the HILs.
Oral and inhalation TRVs are generally derived from direct administration of the chemical to an animal or human and as such they often intrinsically account for ‘bioavailability’ as defined above. TRVs represent tolerable ‘uptake’ or absorbed dose, which is different from total ‘intake’. Uptake is the dose actually absorbed by the body; that is, the amount of the administered dose (or intake) that is bioavailable.
In risk assessments, the dermal pathway has a well-established mechanism for considering absorption and relative bioavailability. The lack of dermal-specific TRVs means that a dermal dose is often compared to the ingestion TRV. However the dermal dose represents an absorbed dose rather than applied dose (as is commonly the case in establishing ingestion TRVs). Hence it may be necessary to modify the ingestion TRV. This is commonly done by applying a gastrointestinal absorption factor (GAF) to the ingestion TRV, which modifies the TRV by a factor that addresses absorption of the chemical across the gastrointestinal tract in the critical toxicity study. For soil-bound contaminants, there is little data on the influence of matrix on dermal absorption. A common approach to address this issue is to apply a dermal absorption factor (DAF) to modify the applied dose in soil to calculate the dermally absorbed dose. It represents the proportion of the contaminant in soil that is considered to be absorbed into the bloodstream through the skin.
TRVs rarely intrinsically account for the relative bioavailability of contaminants in the soil matrix. Established generic values for relative bioavailability in soil are available only for lead (US EPA 2007a). Further discussion on the relative bioavailability of lead considered in the derivation of the HIL is presented in Section 5.4.3. In addition, a relative bioavailability value for arsenic has been considered in the derivation of the HIL. For other contaminants, a relative bioavailability of 100% has been assumed in the derivation of the HILs.
The assumptions noted above with respect to relative bioavailability are relevant to the derivation of HILs only. The conduct of any site-specific risk assessment should further consider site-specific relative bioavailability where relevant (refer to Schedule B4 for further discussion).
A chemical ‘species’ is the specific form of an element defined by its oxidation (valency) state and/or complex or molecular structure. Some of these chemical species are more important for risk assessment than others. In particular, valency state and speciation are of great importance in determining the toxicity of metals and metalloids (WHO 2006).
Cr (VI) and inorganic and organic Hg were considered as separate species in deriving the HILs, but the remainder of the HILs do not account for differences in the toxicity or bioaccessibility/bioavailability of the species of contaminants. Derivation of the HIL required assumptions to be made regarding the form of each metal in soil, and the assumptions made are detailed in the summaries in Appendix A.
A number of HILs represent groups of substances (including carcinogenic PAHs, DDT+DDE+DDD, aldrin and dieldrin, PCBs and PBDEs). Two approaches have been applied to generate a single HIL that represents several contaminants. Where this has been done, directions for application of the HIL are given. The toxicity profile for the group of substances provides details of the assumptions that are inherent in the HIL for the group.
The TEF approach involves the approximation of the properties of a group of similar substances by those of a single member of the group. The components of the mixture are assumed to contribute to the toxicity in a similar way, and their relative effect is calculated in proportion to their concentration in the mixture by adjustment using a relative potency factor. This approach has been applied in the derivation of the HIL for carcinogenic PAHs using benzo(a)pyrene (BaP) as the reference substance.
The toxicity surrogate approach involves the generation of a risk level for a single ‘indicator’ chemical and the application of this information directly to the assessment of other similar chemicals within a group. The sum of all the chemicals in the group is compared to the HIL, assuming that their effect (if more than one of the group is present) is similar and additive. This approach is taken for cresols, PCBs, PBDEs and several groups of pesticides. The approach taken for each substance or group is described in Appendix A.
This section provides an overview of the quantitative model used in the derivation of the HILs, including a description of the model algorithms and a summary of the assumptions, including human behavioural characteristics. The information provided is designed to allow risk assessors to gauge the applicability of the HILs at individual sites.
The approach used in the derivation of the HILs is consistent with the Australian quantitative risk assessment framework, as described in Schedule B4. The calculations undertaken combine data on the toxicity of soil contaminants with estimates of potential exposure by adults and children living, working and/or playing on land affected by contamination, over a specified period. By comparing predicted exposure with toxicity reference values, HILs that are protective of human health have been derived.
The equations used to generate the HILs are presented in Appendix B. The values for all input variables used are provided either within the text, or noted in Appendix A. Appendix C presents all the calculations conducted for the derivation of the HILs using the parameters and assumptions presented in Appendices A and B. In general, values presented within the text are those that are considered most significant in terms of understanding the basis of the HILs. Note that input values related to the blood lead model used to derive the lead HIL are presented in Appendix D.
The exposure pathways addressed in the derivation of HILs include:
The details of the pathways considered for each exposure scenario are presented in Section 3.3.
For each standard exposure scenario, full details of the inherent human assumptions (for example, receptor characteristics and behaviour) are summarised in Table 5. In general, exposure settings were selected for consistency with guidance provided in enHealth (2012a). In some cases the assumptions adopted differ slightly (other than simple rounding differences) from those presented in enHealth (2012a). Consideration of these differences does not change the derived HIL, where the underlying principles for the derivation of HILs outlined in Section 1.4 are adopted.
For the assessment of exposures by young children, the average body weight for a child aged 23 years of 15 kg from enHealth (2012a) has been adopted.
Adults have been assessed on the basis of the average lifetime adult body weight of 70 kg from enHealth (2012a). This body weight is lower than the average adult body weight of 78 kg from enHealth (2012a) and has been selected for the purpose of deriving HILs as it better reflects the larger age range considered for adults in the derivation of HILs (all ages older than a young child aged 05 years) and is consistent with the body weight adopted in the derivation of the Australian Drinking Water Guidelines (NHMRC 2011) and other screening level guidelines developed in New Zealand, the USA, Canada and the Netherlands.
The World Health Organization drinking water guidelines are based on an average adult body weight of 60 kg (WHO 2011), but they are designed to be applicable worldwide and to cater for countries where average body weight would be much lower than that in Australia.
Child exposure duration has been set at 6 years for all land use scenarios, based on the critical child receptor characterised on the basis of exposure parameters for the more sensitive ages of 23 years, but expected to be representative of exposures over all ages from 05 years. Adult residential and recreational exposure duration has been set at 29 years, reflecting total residential exposure duration (child plus adult) of 35 years based on the 95th percentile from enHealth (2012a). An exposure duration of 30 years has been applied for adult commercial receptors as per enHealth (2004).
The exposure frequency applied in the residential and open space scenarios is 365 days/year (enHealth 2012a). This reflects the assumption that exposed populations are potentially using the contaminated site daily; this is a necessary assumption for residential scenarios, but is a worst-case assumption for the recreational scenario. The exposure frequency applied in the commercial/industrial land use scenario is 240 days/year; this value assumes a 5-day working week for 48 weeks/year.
The averaging time selected depends on the type of toxic effect being assessed. The distinction between the approach for threshold and non-threshold compounds relates to the currently held scientific opinion that the mechanism of action differs for these groups (US EPA 1989).
When evaluating chronic exposures (as is the case in the derivation of HILs) to threshold toxicants, intakes are typically calculated by averaging intakes over the period of exposure (essentially the exposure duration multiplied by 365 days in a year). It is noted that the exposure duration cancels out in the exposure equations for threshold compounds.
For non-threshold toxicants, intakes are calculated by averaging the total cumulative dose over a lifetime. This approach for carcinogens is based on the assumption that a high dose received over a short period of time is equivalent to a corresponding low dose spread over a lifetime (US EPA 1989). The convention is almost universally to use an averaging time of a 70-year lifetime, expressed as days, resulting in an estimate of exposure as an annual average daily rate. Hence, for non-threshold contaminants, the averaging time is important.
At birth, the average male in Australia has a life expectancy of 79 years and the average female has an expectancy of 84 years (enHealth 2012b). In fact, according to the 20062008 life tables from the Australia Bureau of Statistics, 88% of females and 81% of males are still alive at age 70. By age 85, these numbers have almost been halved with 40% of males and 56% of females still alive, and these numbers drop rapidly for the next 10 years. Cancer is a disease that can take many years to form, with estimates ranging from 1020 years total. Thus, exposures in the environment that occur into old age are unlikely to have impacts on cancer rates later in life due to the rapid increase in mortality after age 85. Allowing for 1015 years of cancer development, considering lifetime exposure to age 70 would cover the average lifespan for men and women and it would cover most exposure periods where cancers are likely to be initiated. On this basis, the averaging time of 70 years has been retained for carcinogens.
Table 5. Exposure parameters*
Parameter | Symbol (refer to Appendix B) | Units | HIL A residential scenario | HIL B residential scenario | HIL C Open space scenario | HIL D Commercial/industrial scenario | |||
|
|
| Adult | Child | Adult | Child | Adult | Child | Adult |
Body weight | BWA or BWC | kg | 70 | 15 | 70 | 15 | 70 | 15 | 70 |
Exposure duration | EDA or EDC | years | 29 | 6 | 29 | 6 | 29 | 6 | 30 |
Exposure frequency | EF | days | 365 | 365 | 365 | 365 | 365 | 365 | 240 |
Soil/dust ingestion rate1 | IRSA or IRSC | mg/day | 50 2 | 100 2 | 12.5 3 | 25 3 | 25 4 | 50 4 | 25 5 |
Soil/dust to skin adherence factor | AF | mg/cm2/day | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 |
Skin surface area | SAA or SAC | cm2 | 20 000 | 6100 | 20 000 | 6100 | 20 000 | 6100 | 20 000 |
Fraction of skin exposed | Fs | % | 31.5 | 44.3 | 31.5 | 44.3 | 31.5 | 44.3 | 19 |
Dermal absorption factor | DAF | % | Chemical specific values applied | ||||||
Time spent indoors on site each day | ETi | hours | 20 | 20 | 20 | 20 | 0 | 0 | 8 |
Time spent outdoors on site each day | ETo | hours | 4 | 4 | 1 | 1 | 2 | 2 | 1 |
Home-grown fraction of vegetables consumed | FHG | % | 10 | 10 | 0 | 0 | 0 | 0 | 0 |
Vegetable & fruit consumption rate | Cy (veg and fruit) | g/day | 400 | 280 | - | - | - | - | - |
Averaging time for carcinogens (‘lifetime’) | ATNT | years | 70 | 70 | 70 | 70 | 70 | 70 | 70 |
Dust lung retention factor | RF | % | 37.5 | 37.5 | 37.5 | 37.5 | 37.5 | 37.5 | 37.5 |
* A site-specific assessment of risk should be conducted where the exposure scenario differs from the assumptions adopted in the derivation of the HILs (e.g. commercial premises that run continuous 12 hour shifts) | |||||||||
This section summarises the approach and pathway-specific assumptions adopted in the derivation of the HILs. All equations relevant to the calculation of the HILs are presented in Appendix B.
This exposure pathway includes the incidental ingestion of contaminated soil and dust during everyday activities. In addition, the direct consumption of soil adhering to home-grown fruit and vegetables in the residential HIL A exposure scenario has been reviewed. Soil and dust ingestion can be an important exposure pathway for surface soil contaminants and is particularly important in the case of non-volatile chemicals, such as metals. Young children are especially vulnerable to the ingestion of soil contaminants as they may have direct contact with soil and dust during play activities.
Based on a number of overseas tracer studies, enHealth (2012a) recommends default soil (comprising 50% outdoor soil and 50% indoor dust (derived from outdoor soil) as per enHealth (2012b) ingestion rates 100 mg/day for 05 year old children and 50 mg/day for adults. These values have been applied in the derivation of the HILs.
For residential HIL B, the ingestion rates have been taken to be 25% of the total average soil intake to represent ingestion of indoor dust as the main ingestion exposure pathway. This assumes that these residents do not have significant access to on-site communal play areas where ingestion of soil outdoors might be likely. If outdoor recreational/landscaped areas with accessible soil are present, then the more conservative HIL C should be considered for these areas.
Ingestion values for HIL C are calculated assuming that 50% of the total average soil ingestion comes from outdoor soil only.
Ingestion rate for HIL D is calculated assuming that 50% of the total daily soil ingestion occurs while at work on the contaminated site. This allows for a nominal 16-hour waking period during which ingestion occurs (since none occurs while sleeping), 8 hours of which is spent at work.
The HIL assumptions do not include allowance for the small number of children and adults who deliberately eat soil, a behaviour known as ‘soil pica’. Soil pica is a behaviour characterised by repeated intentional soil ingestion and people with soil-pica behaviour may ingest large quantities of soil on a regular basis. Pica behaviour is the deliberate ingestion of non-nutritive substances, such as soil, and can occur in some small children as well as some older children and adults more commonly with severe or profound intellectual disabilities. A number of studies are available that address pica behaviours; however, most of these are associated with substances/materials other than soil such as sand, clay, paint, plaster, hair, string, cloth and paper (and some others). Pica (general) behaviour (incidence) appears to be higher in lower socioeconomic groups, in rural areas, pregnant women, individuals with poor nutritional status and in children and adults with mental illness. US EPA (2008) assumes a default soil ingestion rate of 1 g/day for children with soil pica. It is recommended that a site-specific risk assessment should be considered in situations where soil pica behaviour is likely to occur.
The approach applied to estimate the ingestion rate of soil adhering to home-grown produce was derived from the methodology outlined by the UK Environment Agency (EA 2009e). This approach involves the application of a soil loading factor to account for the adherence of soil to home-grown produce, and a preparation factor to account for the influence of food preparation practices (for example, washing and peeling) on soil loading. The quantity of soil ingested also depends on the amount of home-grown produce consumed. Applying the current UK values to the produce consumption rates assumed relevant for Australia results is the equivalent of an additional soil ingestion rate of approximately 3 mg/day for an adult and 2 mg/day for a child, if 10% of produce is grown at home. This intake is considered only minor in comparison with the soil/dust ingestion rates adopted for adults (50 mg/day) and children (100 mg/day) in HIL A, and is considered to be adequately encompassed within the level of uncertainty inherent in the ingestion rates adopted. Hence, the additional contribution of soil ingested from home-grown produce has not been considered separately in the derivation of HIL A.
Note that the contribution of soil ingested from home-grown produce may be of significance in a site-specific risk assessment where higher intakes of home-grown produce or more site-specific soil/dust ingestion rates are considered.
This exposure pathway considers the dermal uptake of chemicals following skin contact with contaminated soil and dust. Dermal exposure to contaminants is dependent on the following parameters:
The exposure parameters specific to the dermal contact pathway are discussed in detail below.
Clothing reduces dermal contact with contaminated soil. Therefore, the area of exposed skin applied in the derivation of the HILs has been based on the percentage of the skin surface area that is not covered by clothes, on average, under normal Australian circumstances.
enHealth (2012a) provides an estimate of 6100 cm2 for the total skin surface area of a 23-year-old child. An average of 44.3% of this area is estimated to be exposed, based on analysis of the percentage skin surface area not covered during warm weather (that is, the child is wearing shorts or skirt, a short-sleeved shirt and no socks or shoes).
The total skin surface area recommended by enHealth (2012a) for adult exposure is
20 000 cm2. In the residential and open space scenarios, it is assumed that 31.5% of this area is exposed, based on typical clothing worn during gardening and yard work and outdoor recreational activities. In the commercial/industrial exposure scenario, 19% of the adult skin surface area is assumed to be exposed, which is equivalent to only the head, hands and forearms (US EPA 2011).
Dermal exposure to soil contamination is highly dependent on the amount of soil that adheres to the skin following contact. Studies on soil adherence to the skin have shown that it varies according to soil type, the part of the body examined and the type of activities being undertaken when the soil is in contact with the skin; hence, the soil-to-skin adherence factor is a relatively uncertain parameter in any quantitative risk assessment process (US EPA 2004b). The soil-to-skin adherence factor applied in the generation of the HILs was 0.5 mg/cm2, which is the default value recommended by enHealth (2012a).
The process of absorption of chemicals through the skin is described by the dermal absorption factor (DAF), which estimates the percentage of the adhered layer of soil contamination that is able to pass through the skin. The DAF considered in the derivation of the HILs is based on a review of the available data for each compound. It is noted that limited data is available for dermal absorption and hence where data is not available and dermal absorption is of potential significance, default values have been adopted, as described below.
For semi-volatile organic compounds where no compound-specific data is available, a default dermal absorption factor of 0.1 (10%) has been adopted consistent with US EPA Region III (US EPA 1995) and EA (2009e).
Dermal absorption of volatile organics is especially difficult to assess, because most studies have involved occluding (covering) the skin. This may give artificially high skin absorption values, since these compounds would also be expected to volatilise from the skin (MfE 2011a). US EPA Region III recommends using a dermal absorption value of 0.05% for substances with a vapour pressure similar to that of benzene (vapour pressure approximately 95.2 mm Hg). For volatiles which have vapour pressures lower than that of benzene (and where less volatilisation from the skin may occur)—a default skin absorption value of 3% is recommended (US EPA 1995). Review of dermal absorption for benzene by EA (2009f) suggests a value of 1% may be more appropriate. Given the limited data available and the relative insignificance of the dermal absorption pathway for volatile organics, a default of 3% has been assumed in the derivation of HILs, where no other chemical-specific data is available.
The potential significance of dermal absorption and the DAF values adopted in the derivation of HILs are presented for each compound in Appendix A.
Inhalation of dust derived from contaminated soil in both the indoor and outdoor settings has been considered in the derivation of HILs. An assessment of exposure via this pathway depends on three key factors:
For the purpose of developing the HILs for scenarios A, B and D, soil-derived dust concentrations in outdoor air have been calculated using the approach proposed by Cowherd et al. (1985) and adopted by US EPA (2002) and EA (2009e). This approach uses a particulate emission factor (PEF), which relates the concentration of respirable dust particles (diameter <10 µm) in the air with wind speed, vegetative cover and the area of the site occupied by exposed soil. The outdoor dust concentration calculated by this means is assumed to consist of 100% site-derived soil. The value of the PEF depends upon a number of variables that are detailed in Appendix B; of most significance for the relevance of the HIL to a site is the proportion of a site area that is occupied by surface cover (for example, vegetation or hardstand), which is represented by V in Table 6.
Table 6. Proportion of surface cover (V) assumed in HIL scenarios
| HIL A | HIL B residential | HIL D |
Fraction of outdoor surface cover (V) | 0.75 | 0.9 | 0.8 |
For HIL C, dust concentrations have been estimated for more open areas assuming poor ground cover and activities (such as sporting games) that involve the generation of dust. In this case, a dust in air concentration of 39 µg/m3 (95th percentile from Australian data as presented by enHealth 2012a) has been used, where 100% is assumed to be derived from the contaminated site.
For the purpose of deriving the HILs, soil-derived dust concentrations in indoor air have been generally calculated using the approach proposed by EA (2009e). Indoor dust concentrations are assumed to equilibrate with outdoor dust concentrations, as described by the PEF, through natural building ventilation. In addition, indoor air is considered to be enriched with dust compared to the outdoor environment, due to the movement of dust indoors on clothing, footwear, pets, etc. and the potential for the resuspension of dust particles in the indoor environment (EA 2009e). To address this issue, the indoor dust concentration (or dust loading factor) is assumed to be equal to the 95th percentile from Australian data (enHealth 2012a), which is 39 µg/m3.
A significant proportion of house dust can be attributed to soil particles that have been tracked into the indoor environment from outdoors. enHealth (2012a) consider that 50% of the indoor dust is derived from the site soil, in accordance with the recommendations made by US EPA (2008; 2011). This value is the ‘indoor dust transport factor’ (TF), and is the same for all scenarios. The TF is multiplied by an ‘indoor dust loading factor’ (DL) to represent the proportion of this indoor dust (which is largely on the floor) that is resuspended into air by people moving about the building.
Dust particulates are characterised by enHealth (2012a) according to the following particulate size distribution:
The dust lung retention factor describes the percentage of respirable dust that is small enough to be retained in lungs and is associated with health effects. For both indoor and outdoor dust exposures, the respirable fraction is estimated at 37.5% of the inspirable fraction. This fraction is consistent with the fraction considered in the previous HILs (NEPC 1999) and enHealth guidance (enHealth 2004), where it was considered that 75% of the inhaled (inspirable) dust will be retained in the respiratory tract (25% exhaled) of which 50% is small enough to reach the pulmonary alveoli, resulting in a respirable fraction of 37.5%.
This exposure pathway considers exposure to chemical vapours released from soil into indoor and outdoor air. The indoor inhalation of soil-derived vapours is often the most critical exposure pathway for volatile contaminants. Further detail on this exposure pathway is presented in Section 5.5 of this Schedule.
This exposure pathway considers the potential transfer of soil contamination to adults and children, through the consumption of garden vegetables and fruit grown in soils within contaminated sites. This exposure pathway has only been considered in the derivation of the HIL values for the low-density residential setting (HIL A values).
An assessment of exposure via the consumption of home-grown produce depends on these factors:
This last factor is assumed to be 100% for all contaminants, with the exception of lead.
The equations relevant to the assessment of intakes via the consumption of home-grown produce are included in Appendix B.
Vegetable and fruit intakes per day are assumed to be the suggested average intakes presented in enHealth (2012b). A vegetable intake of 100 g/day and a fruit intake of 180 g/day were estimated for a 23-year-old child. The average vegetable and fruit intakes for 1965-year-old adults were estimated to be 260 g/day and 140 g/day respectively.
For the purpose of deriving the HILs, produce has been divided into four categories; green vegetables (for example, lettuce and spinach), root vegetables (for example, carrots and onions), tuber vegetables (for example, potatoes) and fruit. The percentage of vegetable consumption comprised of green, root and tuber vegetables was calculated using data provided by EA (2009e) and is summarised in Table 7.
These percentages were applied to the consumption rates above, resulting in splitting the vegetable consumption rates into rates for the three vegetable categories. The fruit consumption rate could not be split into different kinds of fruit due to lack of data.
Table 7. Percentage of fruit and vegetable consumption comprising separate produce groups
Produce group | Adult residents* (%) | Adult residents consumption Rate** (g/day) | Child residents* (%) | Child resident consumption rate** (g/day) |
Green vegetables | 59 | 153.4 | 55 | 55 |
Root vegetables | 18 | 46.8 | 17 | 17 |
Tuber vegetables | 23 | 59.8 | 28 | 28 |
Tree fruit | 100 | 140 | 100 | 180 |
* Percentage of total vegetables or fruit, from EA (2009e) ** Calculated based on total vegetable and fruit intakes from Australian data (noted above) | ||||
Domestic or backyard food production is a relatively small contributor to overall food production in Australia, with the total annual home-grown fruit and vegetable crop representing 4.1% and 5.3% respectively (ABS 1995). However, a reasonably large proportion of households engage in home food production, with 35% of households producing one or more vegetable types and 36% producing one or more types of fruit (ABS 1995). Any estimate of national behaviour is likely to be somewhat misleading; in particular, the differences between urban and rural populations are likely to be significant.
An average of 10% of vegetable and fruit consumption from home-grown produce has been applied as an appropriate generic estimate for HIL A.
It is noted that the consideration of separate intakes derived for home-grown fruit and vegetable crops in addition to background dietary intakes results in some double counting of fruit and vegetable ingestion and intakes derived from these sources. This has been addressed for each contaminant where plant uptake is considered significant, as noted in Appendix A.
Perhaps the greatest uncertainty in determining uptake of a contaminant in produce is selecting the plant uptake or concentration factors (CFy) (MfE 2011b). Plants can accumulate contaminants via a number of pathways, the most important of which is typically absorption by roots where, depending on the nature of the contaminant, translocation to other portions of the plant may occur. Uptake of organic contaminants and metals occurs predominantly from the soil solution. Normally the concentration of a contaminant measured in the soil solution represents only a fraction of the total contaminant present in the soil. The ratio of the concentration in soil solution to the total in soil depends on a number of factors including soil pH, redox potential, soil organic matter, and soil texture. In soils and sediments where the clay content is relatively low, the availability of organic contaminants is strongly related to the fraction of organic carbon present (MfE 2011b).
Review of plant uptake models/approaches by MfE (2011b) indicated that, for organics, a range of simple and complex models are available. The review notes work done by EA (2006) where a number of models for the uptake of organic compounds in plants were reviewed.
A number of limitations were identified including the limited range of compounds tested (namely PAHs, PCBs and dioxins) and problems with study data (in reporting dry or fresh weight and whether data was from roots, shoots, fruits or tubers), highlighting the level of caution that should be considered in applying these models. Overall, the EA (2006) review concluded that the model performance was highly variable and all but one model over-predicted root uptake by at least an order of magnitude.
On this basis, MfE recommended to simply use CFs based on available data, and only resort to models (for organic compounds only) when measured values are not available. This approach has been adopted in the derivation of HIL A.
For metal contaminants and other inorganics (except cyanide), default values of CFx for As, Cd Ni, Hg and Se have been derived from detailed reviews provided by the EA (EA 2009a, 2009b, 2009c, 2009d). The potential significance of plant uptake and the approach adopted for other metals has been addressed on a compound-specific basis in Appendix A.
For organic contaminants (where relevant), soil-to-plant concentration factors (CFy) have been calculated according to the algorithms described by EA (2009e) and summarised in Appendix B. With the exception of the assumption regarding the fraction of soil organic carbon, assumptions about soil properties are generally the same as those used in the vapour pathway, and are described elsewhere in this Schedule. The contaminant-specific physical and chemical properties are given in the relevant toxicity profile in Appendix A.
An assumption of 0.3% organic carbon has been applied to the vapour intrusion exposure pathway for the interim HILs for VOCCs, as this value is consistent with the characteristics of an average sandy soil, as defined by US EPA (2004a). An assumption of 2% organic carbon has been applied only to the calculation of CFy values, due to likely increases in soil organic carbon levels following the long-term cultivation of home-grown produce.
Blood lead levels are considered to be the best index of lead exposure and risk in humans. For this reason, the HILs for lead are calculated using a different approach from that for all other HILs. For the purpose of deriving the HILs, lead has been assumed to act as a threshold contaminant and a blood lead concentration of 10 µg/dL has been applied, as all Australians should have a blood lead level below this level (NHMRC 2009). It should be noted that it is generally recognised that there may be no threshold for the neurotoxic action of lead (DEFRA 2002).
Adult exposures to lead have been estimated based upon the methodology developed by US EPA (2003) as provided in the US EPA adult lead model. This methodology is focused on estimating blood lead concentrations in female adults exposed to lead-contaminated media and the transfer of blood lead to the unborn foetus. The adult blood lead model incorporates lead exposure, uptake into the body and biokinetic transfer into the blood and developing foetus.
The adult lead intake rate (dominated by soil ingestion) is calculated. The estimated adult exposure is then converted to a blood lead concentration. The equation applied in the transfer of lead into adult blood and into the developing foetus is based on the methodology provided in US EPA (2003) and is given below.
PbBadult | = | PbBbackground | + | Pbintake x BKSF x EF |
|
|
|
| AT |
where
PbBadult | = total adult blood lead concentration from all sources (µg/dL) |
AT | = averaging time (days/year) |
EF | = exposure frequency (days/year) |
PbBbackground | = background adult blood lead concentration (µg/dL) |
Pbintake | = total lead uptake from all media (g/day) |
BKSF | = biokinetic slope factor (µg/dL per µg/day) |
This approach allows for protection of the most sensitive receptor in the adult scenario, which is an unborn child carried by a pregnant mother.
Child exposure to lead has been estimated using the integrated exposure uptake biokinetic model for lead in children (IEUBK model, version 1.1 Build9, released June 2009) developed by the US EPA in 2002 and described by US EPA (1998, 2007b).
The IEUBK model comprises separate components for exposure, absorption and the biokinetic transfer of lead to all tissues of the body and calculates age-specific blood lead concentrations for children aged between 0 and 7 years. The HILs are based on the age range 12 years, as this age is considered to be the most sensitive as a result of lowest body weight combined with high hand-to-mouth activity and crawling.
The components of the IEUBK model can be summarised as follows:
The model contains 100 variables, of which 46 can be modified by the user. Those which cannot be modified are based on considerable research, and are detailed in the model user guide (US EPA 2007b). In calculating the HILs for lead, input variables consistent with those used for the other HILs have been applied. A full list of variables input to the model is provided in Appendix D, including important variables where the model defaults were retained.
Lead is the only substance for which adequate data is available to support an estimate of bioavailability. Because the toxicity criterion in lead modelling is a blood lead value, it represents an absorbed quantity and estimation of both bioavailability and bioaccessibility is appropriate. A single factor, labelled ‘bioavailability’ is used to represent both concepts.
US EPA (2007a) recommends use of 30% oral bioavailability of lead in soil for children, and 12% bioavailability of lead in soil for adults. There is also data available from Australian sites, which indicate that an oral bioavailability of at least 45% is likely (David Simon, South Australia Health, pers comm.).
Following review of the available data, an oral bioavailability of 50% (based on a review of data presented by IARC (2006)) was used in the models used for the derivation of an HIL associated with exposures to lead.
The inhalation of vapours in the indoor and outdoor environment is an important exposure pathway for volatile and semi-volatile soil contaminants. The approach adopted for the derivation of HILs has used an empirical approach using an attenuation factor, rather than a model, for estimating concentrations indoors and outdoors from soil vapours. There are a number of limitations and uncertainties associated with the use of any model in the estimation of exposure concentrations. In particular, the methodology and uncertainties associated with vapour modelling from a soil source are not fully resolved.
Hence, at this stage for VOCCs, investigation levels have only been derived for soil vapour concentrations (where the soil vapour is the most appropriate data (direct measurement) for the assessment of exposure) and are considered interim HILs. The further development of HILs for these compounds will rely on improvements in understanding of the behaviour of chlorinated hydrocarbons in transferring from soil and soil vapour to indoor and outdoor air.
With respect to the measurement of volatile compounds in soil vapour, readers are referred to Schedule B2 and Davis et al. (2009) for field assessment methods for vapours.
All equations relevant to the derivation of the interim HILs for soil vapour are presented in Appendix B and in the HILs spreadsheet available from the ASC NEPM Toolbox.
The interim soil vapour HILs for VOCCs are dominated by the vapour migration and intrusion (to indoor air) pathway. The quantification of vapour migration from the source (or point of measurement) to the point of exposure (indoors) requires an assessment of migration (via diffusion and/or advection) through overlying soil and into a building where it mixes within the building (including mixing as the building air is exchanged with ambient air). Other processes that limit/retard the migration of vapours (such as sorption, transformation and degradation) or enhance vapour migration (such as via preferential pathways) also occur, though these have not been considered in the HILs. Consequently the interim soil vapour HILs are conservative.
The movement of soil vapour into a building can be described on the basis of an attenuation factor (α), which is the ratio of the indoor air vapour concentration to the soil vapour concentration.
The approach adopted for the derivation of interim HILs has involved the use of an indoor air to soil vapour attenuation factor (or ratio). US EPA (2012a) has summarised measured attenuation factors (based on data from a range of residential sites) between indoor air and groundwater, external soil vapour, sub-slab vapour and crawl-space vapour concentrations.
The attenuation factors have been collated by US EPA (2012a) across a range of soil types and building types that include both slab and basement construction. The evaluation conducted by US EPA has considered the influence of background sources. Hence they are relevant for consideration in the derivation of generic HILs relevant for a wide range of sites. The use of these attenuation factors requires no further modelling of the vapour from the source (or point of measurement) to the point of exposure in indoor air.
The evaluation of the data sets referenced by US EPA only relates to the assessment of chlorinated hydrocarbon vapours, which is relevant to the derivation of the interim HILs. The potential for vapour intrusion risks for chlorinated hydrocarbons differs from that for petroleum hydrocarbons (US EPA 2012b) and hence the approach adopted in deriving interim HILs for chlorinated compounds should not be applied to other volatile compounds (in particular petroleum hydrocarbons) without consideration of chemical-specific issues such as the potential for biodegradation. Chlorinated hydrocarbons are recalcitrant (i.e. do not degrade) in the presence of oxygen, unlike petroleum hydrocarbons, which are readily biodegradable in the presence of oxygen.
The following figure is an extract from US EPA (2012a), which presents these measured attenuation factors.

Figure 5. Summary of attenuation factor distributions for groundwater, external soil vapour, sub-slab, and crawlspace for chlorinated hydrocarbon vapours (ref: US EPA 2012a, Figure 34)
For sub-slab soil vapour attenuation factors for all residential premises, the measured values ranged from 0.00003 to 1, with a median value of 0.003 and a 95th percentile of 0.03. For soil vapour data collected external to an existing residential building (i.e. not directly beneath the building) there is a wider variation in attenuation factors, ranging from 0.00005 to 1.3, with a median value of 0.004 and 95th percentile of 0.3.
A conservative attenuation factor of 0.1 (which is towards the 95th percentile of the US EPA database) has been adopted for the derivation of soil vapour HILs where the pathway of vapour migration is from subsurface (sub-slab or shallow soil vapour) to indoor air for residential and commercial buildings. This decision was based on the available attenuation factors for chlorinated compounds presented by US EPA (2012a), the recalcitrant nature of most chlorinated hydrocarbons in aerobic environments and consideration of the underlying principles for deriving HILs outlined in Section 1.4 (in particular to embody a margin of safety for most exposure scenarios).
Inhalation indoors is the only significant pathway of concern considered for residential A, B and commercial D scenarios. The soil vapour interim HIL has been calculated on the basis of the equations presented in Appendix B, which uses exposure parameters relevant for the quantification of exposures by residents (HILs A and B) and workers (HIL D).
It is recognised that adopting 0.1 as the set attenuation factor will be very conservative for a number of sites where additional attenuation may occur, for example, sites with deeper sources of vapours or sites with higher building air exchange rates, or where other attenuation mechanisms (including biodegradation) may occur.
The derived soil vapour interim HILs do not address crawl-space buildings or the presence of preferential vapour pathways.
In relation to preferential pathways, most sites comprise subsurface materials with highly variable permeability as well as a number of subsurface utility penetrations. Of particular concern in relation to vapour intrusion are utilities (as illustrated in Figure 6) or geologic features (such as fractures or highly permeable materials) that intersect a vapour source and connect to a building (ITRC 2007: API 2005). In these cases the soil vapour interim HILs may not be adequately protective and a site-specific assessment should be undertaken.

Figure 6. Preferential vapour transport through utility trench (ref: US EPA 2012b, Figure 5)
The assessment of inhalation exposures associated with outdoor air is of most significance to the derivation of HILs for open space/recreational areas (HIL C). Limited information is available on attenuation factors relevant for outdoor air. The concentrations in outdoor air, which are derived from the migration of vapours from a subsurface source, are expected to be lower than those indoors due to increased dilution, particularly during the daytime.
Review of average radon data suggests that outdoor air concentrations are in the order of 2 to 10 times lower than indoor air concentrations (ECA 1995). Based on this information, the more conservative ratio of indoor air to outdoor air concentrations above a subsurface source of 2 has been considered. This allows for the consideration of outdoor exposures that may occur in areas where less dilution occurs, including sunken sandpits/play areas (and includes cubby houses). It is considered likely that dilution will be higher, however without more sound data that addresses a wide range of outdoor exposures it is not considered appropriate for screening level guidance to be less conservative. Hence, the attenuation factor adopted for the estimation of outdoor air concentrations is 0.05 (half that of the indoor air attenuation factor).
The soil vapour interim HIL C has been calculated on the basis of the equations presented in Appendix B.
As with the estimation of indoor exposures, it is recognised that adopting 0.05 as the soil vapour to outdoor air attenuation factor does not take into account additional attenuation that may occur for sites with deeper sources of vapours, windier environments, or where other attenuation (including biodegradation) may occur. Consideration of these issues should be included in a site-specific assessment.
Risk characterisation is the process through which the results of the exposure assessment and toxicity assessment processes are combined to provide numerical estimates of the potential risks to the identified receptors. The HILs have been calculated on the basis of the equations using a threshold or non-threshold approach, as appropriate. The HILs are presented in Appendix B, with the calculations presented in Appendix C. The HILs have been derived for each compound assuming intakes from all pathways of exposure are additive.
The derivation of HILs, using the equations presented in Appendix B, requires the consideration of a target risk level for threshold and non-threshold calculations.
For threshold HIL calculations, a target hazard index (HI, which is the ratio of the intake of a contaminant from all sources (including the site) to the threshold TRV) over all pathways of exposure (where relevant) of 1 has been adopted. This is consistent with the discussion presented in Schedule B4.
For non-threshold HIL calculations, a tolerable (or target) incremental lifetime cancer risk associated with intakes of a contaminant (derived from a contaminated site) via all pathways of exposure of 1x10-5 has been adopted (see Schedule B4).
Tolerable incremental lifetime cancer risk values available from Australia and international agencies (refer to discussion in Schedule B4) range from 1x10-4 to 1x10-6, with the value of 1x10-5 generally adopted for the assessment of contaminated land issues in a number of individual states in Australia. The lower incremental lifetime cancer risk values (1x10-6) are commonly adopted in guidance that addresses population-wide exposures, such as those that may be derived from drinking water (and considered in the current Australian Drinking Water Guidelines (NHMRC 2011)).
The HILs presented have been rounded to one, and no more than two, significant figures (as shown in Appendix C). The rounding reflects the level of uncertainty inherent in the range of variables used to define exposure and doseresponse. Some further discussion on uncertainty is presented below.
The uncertainty analysis is a qualitative process that identifies the key assumptions and data gaps associated with a human health risk. Uncertainty can arise from missing or incomplete information, or arise from the scientific theory affecting the ability of a model to make predictions or result from uncertainty affecting a particular exposure or input parameter. Uncertainty has the potential to result in a cumulative overestimation or underestimation of potential health risks during an assessment.
The three broad types of uncertainty inherent in any risk assessment are:
Scenario uncertainty in the HIL assessment is largely not applicable, since the circumstances of the assessment are hypothetical.
There is considerable parameter uncertainty in the HIL assessment. Parameter uncertainty is usually dealt with by sensitivity analysis (see below); however, because of the generic purpose of the HILs, many of the parameters for tier 1 assessment are set, for example by enHealth (2012a, 2012b), and sensitivity analysis for these was not considered appropriate. The approach used to address parameter uncertainty during the derivation of the HIL values was the use of conservative or reasonable high-end exposure assumptions, allowing them to be applied across the majority of Australian sites.
Assumptions applied during the development of the HILs include:
The models used to estimate exposure are inherently uncertain, and are not necessarily able to accurately predict actual exposure. The soil and dust ingestion, vapour inhalation, and dermal pathway approaches/models are well established and have been in use in international risk assessment for many years. Although quantitatively they may not be very good absolute predictors of exposure, they are very simple and primarily dependent on the exposure settings and toxicity criteria.
The pathways most subject to model uncertainty were the concentration of contaminants in vegetables and fruit, and the prediction of airborne dust concentrations. Uncertainty analysis was carried out by evaluating the pathways driving the HIL values (that is, percentage contributed by each) and assessing the likely reality of the proportions of exposure from each pathway. In the case of both the vegetable uptake and airborne dust pathway a number of contaminants showed unrealistic proportions of exposure. Further consideration of the model assumptions and algorithms in both cases led to the conclusion that sensitivity to input values, rather than problems with the algorithms, was the cause. The subsequent sensitivity analysis is described below.
Site-specific exposure scenarios provide the most reliable information for assessing potential human health risks. In order to allow the HIL values to be applied across a variety of Australian sites, however, generic scenarios were applied to estimate the magnitude of potential exposure.
In sensitivity analyses, the values of parameters suspected to drive exposure risks are varied and the degree to which changes in the input variables result in changes to the risk estimates are summarised and compared (US EPA 1989). Throughout the process of deriving the HILs, sensitivity analyses were performed to provide a ‘reality check’ for the data adopted and to identify the key parameters influencing the resultant HIL values.
The HIL values for all of the contaminants of concern are sensitive to both the toxicity criteria and background exposure allocation applied in the risk characterisation model. Similarly, human behavioural factors such as body weight, exposure frequency and duration have a significant effect on the HIL value derived. Those assumptions derived from enHealth (2012a) were not varied, since these were considered policy decisions. Other exposure parameters identified as having a significant influence on the derived HIL values differ according to the physicochemical characteristics of the contaminants and, in particular, the volatility of the individual chemicals. The approach taken for the key sensitive parameters is broadly summarised below.
The vegetable ingestion pathway is highly sensitive to Foc. Friebel and Nadebaum (2011) selected a value of 0.3% organic carbon based on data for subsurface soils from ANRA (2001) in the derivation of petroleum HSLs since many contaminated sites, particularly development sites, have been stripped of their more organic-rich topsoils. However, this value proved unsuitable for use with the vegetable ingestion pathway, resulting in unrealistic exposure percentages deriving from vegetables. While the underlying reason for this effect is in the model formulation, increasing the Foc produced much more realistic results. It was also considered unlikely that vegetables and fruit would actually be cultivated in soils with an organic carbon content as low as 0.3% and a value of Foc= 2% was selected to apply to the vegetable pathway. In areas where lower levels of organic carbon are present in soil in the root zone, this needs to be considered in a more site-specific assessment for organic contaminants of concern. The Foc does not affect the assessment of plant uptake of inorganic compounds; however it is important for organic compounds.
The assessment of vapour intrusion for volatile organic chlorinated compounds (VOCC) has not been conducted using a model; rather, it is based on measured soil vapour and indoor air concentrations and associated attenuation factors. The measured attenuation factors range over several orders of magnitude reflecting the wide range of sites and conditions included in the database. Indoor and outdoor air exposure concentrations are linearly related to the attenuation factor used. Hence, the adoption of an attenuation factor that is ten times lower will result in an indoor or outdoor air exposure concentration that is ten times lower, and an interim soil vapour HIL that is ten times higher.
ABS 1995, National Nutrition Survey: Nutrient Intakes and Physical Measurements, Cat. no. 4805.0, Australian Bureau of Statistics, Commonwealth of Australia.
ANRA 2001, Australian Agricultural Assessment 2001, Australian Natural Resources Atlas, http://www.anra.gov.au/topics/agriculture/pubs/national/agriculture_contents.html.
API 2005, Collecting and interpreting soil gas samples from the vadose zone. A Practical Strategy for Assessing the Subsurface Vapor-to-Indoor Air Migration Pathway at Petroleum Hydrocarbon Sites. Regulatory and Scientific Affairs, API Publication 4741, American Petroleum Institute, Washington, DC, USA.
CCME 2008, Canadian Soil Quality Guidelines for Carcinogenic and Other Polycyclic Aromatic Hydrocarbons (Environmental and Human Health Effects), Canadian Council of Ministers of the Environment, Scientific Supporting Document, 218 pp.
Cowherd, C, Muleski, GE, Englehart, PJ & Gillette, DA 1985, Rapid assessment of exposure to particulate emissions from surface contamination sites, EPA/600/8-85/002, United States Environmental Protection Agency, Washington, DC.
Davis, GB, Wright, J & Patterson, BM 2009, Field assessment of vapours, CRC CARE Technical report no. 13, CRC for Contamination Assessment and Remediation of the Environment, Adelaide, Australia.
DEFRA 2002, Contaminants in soil: collation of toxicological data and intake values for humans; lead, R&D Publications, TOX6, Department for Environment Food and Rural Affairs, UK.
Department of Resources, Energy and Tourism 2008, Leading Practice Sustainable Development Program for the Mining Industry: Cyanide Management, Australian Government, Department of Resources, Energy and Tourism, May 2008.
EA 2006, Evaluation of models for predicting plant uptake of chemicals from soil, Science report SC050021/SR, Environment Agency, Bristol, UK.
EA 2008, Compilation of data for priority organic pollutants for derivation of soil guideline values, Science report SC050021/SR7, Environment Agency, Bristol, UK.
EA 2009a, Soil guideline values for inorganic arsenic in soil, SC050021/arsenic SGV, Environment Agency, Bristol, UK.
EA 2009b, Soil guideline values for mercury in soil, SC050021/mercury SGV, Environment Agency, Bristol, UK.
EA 2009c, Soil guideline values for nickel in soil, SC050021/ nickel SGV, Environment Agency, Bristol, UK.
EA 2009d, Soil guideline values for selenium in soil, SC050021/selenium SGV, Environment Agency, Bristol, UK.
EA 2009e, Updated technical background to the CLEA model, Science report SC050021/SR3, Environment Agency, Bristol, UK.
EA, 2009f, Soil guideline values for benzene in soil, SC050021/benzene SGV, Environment Agency, Bristol, UK.
ECA 1995, lndoor air quality and its impact on man, radon in indoor air, Report no. 15, EUR 161 23 EN, European Collaborative Action, Office for Official Publications of the European Community, Luxembourg.
enHealth 2004, Environmental health risk assessment; guidelines for assessing human health risks from environmental hazards, Department of Health and Ageing and enHealth Council, Canberra, Australia.
enHealth 2012a, Environmental health risk assessment; guidelines for assessing human health risks from environmental hazards, Environmental Health Subcommittee (enHealth) of the Australian Health Protection Principal Committee, Canberra, Australia.
enHealth 2012b, Australian exposure factor guidance. Environmental Health Subcommittee (enHealth) of the Australian Health Protection Principal Committee, Canberra, Australia.
Friebel, E & Nadebaum, P 2011, HSLs for petroleum hydrocarbons in soil and groundwater, part 1: technical development document, Technical report no. 10, CRC for Contamination Assessment and Remediation of the Environment, Adelaide, Australia.
Health Canada 2004, Federal contaminated site risk assessment in Canada, part 1: guidance on human health preliminary quantitative risk assessment (PQRA), Ottawa, Canada.
IARC 2006, IARC monographs on the evaluation of carcinogenic risks to humans, inorganic and organic lead compounds, vol. 87, IARC Press, International Agency for Research on Cancer, Lyon, France.
ICMI 2009, Auditor Guidance for Use of the Gold Mining Operations Verification Protocol, International Cyanide Management Institute, October 2009, 4.0 Operations, Standard of Practice 4.5.
IPCS 2004, IPCS Risk Assessment Terminology, International Programme on Chemical Safety, http://www.inchem.org/documents/harmproj/harmproj/harmproj1.pdf.
ITRC 2007, Vapor Intrusion Pathway: A Practical Guide, Technical and Regulatory Guidance, January 2007, Interstate Technology & Regulatory Council, Vapor Intrusion Team.
MfE 2011a, Toxicological intake values for priority contaminants in soil, New Zealand Ministry for the Environment, Wellington, New Zealand.
MfE 2011b, Methodology for deriving soil guideline values protective of human health, New Zealand Ministry for the Environment, Wellington, New Zealand.
NEPC 1999, National Environment Protection (Assessment of Site Contamination) Measure, National Environment Protection Council.
NEPC 2003, Proceedings of the 5th national workshop on the assessment of site contamination, by Langley,A, Gilbey, M & Kennedy, B, May 2003.
NEPC 2006, National Environment Protection (Assessment of Site Contamination) Measure: Review report, National Environment Protection Council.
NHMRC 2009, Blood lead levels for Australians: information paper, National Health and Medical Research Council. (Available online at http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/gp2-lead-info-paper.pdf).
NHMRC 2011, National water quality management strategy. Australian drinking water guidelines, National Health and Medical Research Council, Australia.
RIVM 2001, Risk assessment of historical soil contamination with cyanides: origin, potential human exposure and evaluation of intervention values, RIVM Report 711701019, National Institute of Public Health and the Environment, Bilthoven, Netherlands.
US EPA 1989, Risk assessment guidance for Superfund, volume I: Human health evaluation manual (Part A), Interim final report, EPA/540/1-89/002, Office of Emergency and Remedial Response, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 1992, Supplemental guidance to RAGS: calculating the concentration term, 9285.7-08, Office of Solid Waste and Emergency Response, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 1995, Technical Guidance Manual, Assessing Dermal Exposure from Soil. US EPA Region 3, December 1995, available from:
http://www.epa.gov/reg3hwmd/risk/human/info/solabsg2.htm.
US EPA 1998, The conceptual structure of the integrated exposure uptake biokinetic model for lead in children, Environmental health perspectives supplements, 106; S6, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 2002, Supplemental guidance for developing soil screening levels for Superfund sites, OSWER 9355.4-24, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 2003, Recommendations of the technical review workgroup for lead - an approach to assessing risks associated with adult exposure to lead in soil, , EPA/540/R-03/001, Technical Working Group for Lead, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 2004a, Users guide for evaluating subsurface vapour intrusion into buildings, Office of Emergency and Remedial Response, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 2004b, Risk assessment guidance for Superfund, vol. 1: Human health evaluation manual (Part E) supplemental guidance for dermal risk assessment, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 2007a, Guidance for evaluating the oral bioavailability of metals in soils for use in human health risk assessment, OSWER 9285.7-80, United States Environmental Protection Agency, Washington, DC,USA.
US EPA 2007b, Users guide for the integrated exposure uptake biokinetic model for lead in children (IEUBK), EPA/9285.7-42, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 2008, Child-specific exposure factors handbook, Final report, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 2011, Exposure factors handbook: 2011 update. EPA/600/R-090/052F, September 2011, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 2012a, EPA’s Vapor Intrusion Database: Evaluation and Characterisation of Attenuation Factors for Chlorinated Volatile Organic Compounds and Residential Buildings, EPA/530/R-10/002, March 16 2012, United States Environmental Protection Agency, Washington, DC, USA.
US EPA 2012b, Petroleum Hydrocarbons and Chlorinated Hydrocarbons Differ in their Potential for Vapor Intrusion, Office of Underground Storage Tanks, United States Environmental Protection Agency, Washington, DC, USA, March 2012.
WHO 1998, Environmental Health Criteria 202, Selected Non-Heterocyclic Polycyclic Aromatic Hydrocarbons, International Programme on Chemical Safety – Geneva, World Health Organization.
WHO 2006, Elemental speciation in human health risk assessment, Environmental health criteria 234, World Health Organization, Geneva.
WHO 2011, Guidelines for drinking-water quality, 4th edn, World Health Organization, Geneva.
Acceptable daily intake (ADI) of a chemical that, during a lifetime, appears to be without appreciable risk, on the basis of all the facts known at the time. It is expressed in milligrams per kilogram of body weight per day (mg/kg/day). For this purpose ‘without appreciable risk’ is taken to mean that adverse effects will not result even after a lifetime of exposure. |
Acceptable risk is a risk management term. The acceptability of risk depends on scientific data, social, economic and political factors, and the perceived benefits arising from exposure to an agent. |
Acute exposure is contact between a chemical substance and a target occurring over a short time, generally 14 days or less, with a single or repeated dose. Other terms, such as ‘short-term exposure’ are also used. |
Adverse effect is a change in the morphology, physiology, growth, development, reproduction, or life span of an organism, system, or population that results in an impairment of functional capacity, an impairment of the capacity to compensate for additional stress, or an increase in susceptibility to other influences. |
Agent is any chemical, physical or biological substance or factor (including social factor) being assessed in the context of an environmental health risk assessment. |
Aliphatic is a hydrocarbon compound that does not contain a benzene ring. Aliphatic compounds may be straight, branched or cyclic chains of carbon atoms. They may include double or triple bonds. Carbon atoms in the chain are also generally bonded to hydrogen atoms but other elements, for example, chlorine, sulphur and nitrogen can also be present. |
Aromatic is a hydrocarbon compound containing one or more benzene rings. |
Background concentrations means the naturally occurring, ambient concentrations of substances in the local area of a site. |
Bioaccessibility is the fraction of a contaminant in an exposure medium that is soluble in the relevant physiological milieu (usually the gastrointestinal tract) and available for absorption. Generically, it is the ability for a chemical to come into contact with the absorbing surfaces in an organism. It is related to solubility and dissolution, since absorption usually can only occur from a liquid or gaseous phase and not from a solid phase. |
Bioavailability is a generic term defined as the fraction of a contaminant that is absorbed into the body following dermal contact, ingestion or inhalation. It is expressed as the ratio (or percentage) of the absorbed dose (systemic dose) to the administered dose. |
Cancer is a disease of heritable, somatic mutations affecting cell growth and differentiation; that is, genetic alterations incurred in the first damaged cells are acquired in subsequent cells after cell division within the same individual. |
Cancer slope factor is the plausible upper-bound estimate of the probability of a carcinogen response per unit of intake of a chemical substance over a lifetime. |
Carcinogen is a cancer-causing chemical substance/agent. A distinction may be made based on the presumed mode of action (MoA) – see genotoxic and non-genotoxic. |
Chemical substance means any organic or inorganic substance, whether liquid, soil or gaseous. |
Chemical of potential concern is a chemical substance that is potentially site-related and whose data is of sufficient quality to be judged as potentially causing an adverse health effect. |
Chronic exposure is a continuous or intermittent long-term contact between a chemical substance and a target. |
Clean-up level is a concentration of contaminant in soil or water derived for the purpose of providing an acceptable standard for remediation. May be risk-based or modified by considerations of feasibility, practicality, acceptability, timescale and cost. |
Concentration is the amount of material or agent dissolved or contained in unit quantity in a given medium or system. |
Conceptual site model (CSM) is the description of a site including the environmental setting, geological, hydrogeological and soil characteristics together with the nature and distribution of contaminants. Potentially exposed populations and exposure pathways are identified. Presentation is usually graphical or tabular with accompanying explanatory text. |
Contact volume is a volume containing the mass of a chemical substance that contacts the exposure surface. |
Contaminant is any chemical existing in the environment above background levels and representing, or potentially representing, an adverse health or environmental risk. |
Contamination means the condition of land or water where any chemical substance or waste has been added as a direct or indirect result of human activity at above background level and represents, or potentially represents, an adverse health or environmental impact. |
Critical effect is the adverse effect judged to be the most appropriate for determining the tolerable intake. It is usually the most sensitive adverse effect, that is, that with the lowest effect level, or sometimes a more severe effect, not necessarily having the lowest effect level. |
Data quality objectives (DQOs) describe the establishment of the amount, nature and quality of data required to complete a specific risk assessment. Default value is a pragmatic, fixed or standard value used in the absence of relevant data. |
Dose is the stated quantity or concentration of a substance to which an organism, system or population is exposed over a continuous or intermittent duration of exposure. It is generally the total amount of a chemical administered to, taken up by, or absorbed by an organism, system, or population. |
Doseresponse curve is a graphical representation of a doseresponse relationship. |
Doseresponse is the relationship between the amount of chemical administered to, taken up by, or absorbed by an organism, system, or population and the change developed in that organism, system, or population in reaction to the agent. |
Effect is the change in the state or dynamics of an organism, system, or population caused by exposure to a chemical. |
Expert/professional judgement is the opinion of an authoritative person on a particular subject. |
Exposed population are the people who may be exposed to the contaminant. Synonymous with ‘receptor’. |
Exposure assessment is the evaluation of the exposure of an organism, system, or population to a chemical (and its derivatives). |
Exposure is the concentration or amount of a particular chemical that reaches a target organism, system or population at a specific frequency for a defined duration. |
Exposure concentration is the exposure mass divided by the contact volume or the exposure mass divided by the mass of contact volume, depending on the medium. |
Exposure duration is the length of time over which continuous or intermittent contacts occur between a chemical and the exposed population. |
Exposure event is the occurrence of continuous contact between a chemical and an exposed population. |
Exposure frequency is the number of exposure events within an exposure duration. |
Exposure model is a conceptual or mathematical representation of the exposure process. |
Exposure pathway is the means by which a contaminant makes contact with the exposed population. |
Exposure route is the way in which a chemical substance enters a target after contact (for example, ingestion, inhalation or dermal absorption). |
Exposure scenario is a set of conditions or assumptions about sources, exposure pathways, concentration of contaminants involved, and exposed population (that is, numbers, characteristics, habits) used in the evaluation and quantification of exposure(s) in a given situation. |
Genotoxic chemicals are those for which there is adequate evidence of the potential to interact with, and/or modify the function of genetic material and which have the ability to induce tumours via a mechanism involving direct damage to DNA. |
Hazard is the inherent property of a contaminant or situation having the potential to cause adverse effects when a population may be exposed to that contaminant. Hazard identification is the identification of the type and nature of adverse effects where a contaminant has an inherent capacity to cause harm to an exposed population. |
Hazard index (HI) is the sum(s) of at least two hazard quotients. It is noted that WHO is moving towards the use of risk indices (RI). |
Hazard quotient (HQ) is the ratio of the mean daily intake to the reference dose or tolerable daily intake for threshold exposure. It is noted that WHO is moving towards the use of risk quotients (RQ). |
Health investigation levels (HILs) mean the concentration of a contaminant above which further appropriate investigation and evaluation will be required to ensure the protection of human health. |
Health risk assessment (HRA) is the process of estimating the potential impact of a chemical, biological or physical agent on a specified human population system under a specific set of conditions. |
Health risk management is the process of evaluating and implementing appropriate options to address risks identified from health risk assessments. The decision-making will incorporate scientific, social, economic and political information. |
Intake is the total amount of contaminant (or dose) taken into the body by the exposure route. Multiple-lines-of-evidence approach is the process for evaluating and integrating information from different sources of data and uses best professional judgement to assess the consistency and plausibility of the conclusions that can be drawn. |
Non-aqueous phase liquid (NAPL) is a chemical substance that is insoluble or only slightly soluble in water, which exists as a separate liquid phase in environmental media. The free liquid phase of a chemical substance, which is not dissolved in water or adsorbed to soil. |
Non-genotoxic carcinogen is a chemical substance which induces tumours via a mechanism which does not involve direct damage to genetic material (DNA). |
Pica is a behaviour exhibited occasionally by young children and rarely by adults, characterised by the deliberate ingestion of non-nutritive substances, such as soil. Habitual or repetitive pica specifically involving soil-eating behaviour (or ‘geophagia’) is uncommon. |
Reference dose is an estimate of the daily exposure dose that is likely to be without deleterious effect even if continued exposure occurs over a lifetime. Equivalent in meaning to tolerable daily intake and acceptable daily intake. |
Remediation is the cleaning up or management of contamination. |
Response is change developed in the state of dynamics of an organism, system, or population in reaction to exposure to a chemical substance. |
Risk means the probability in a certain timeframe that an adverse outcome will occur in a person, a group of people, plants, animals and/or the ecology of a specified area that is exposed to a particular dose or concentration of a chemical substance, that is, it depends on both the level of toxicity of the chemical substance and the level of exposure to it. Risk differs from hazard primarily because risk considers probability. |
Risk assessment is the process of estimating the potential impact of a chemical, physical, microbiological or psychosocial hazard on a specified human population or ecological system under a specific set of conditions and for a certain timeframe. |
Risk characterisation is the qualitative, and wherever possible, quantitative determination, including attendant uncertainties, of the probability of occurrence of known and potential adverse effects of a contaminant on a given organism, system or population, under defined exposure conditions. |
Risk communication is an interactive exchange of information about health and environmental risks amongst risk assessors, managers, news media, interested groups, and the general public. |
Risk estimation is the quantification of the probability, including attendant uncertainties, that specific adverse effects will occur in an organism, system, or population due to actual or predicted exposure. |
Risk evaluation is the establishment of a qualitative or quantitative relationship between risks and benefits of exposure to a chemical, involving the complex process of determining significance of the identified hazards and estimated risks to the system concerned or affected by exposure. Risk evaluation is an element of risk management. Risk evaluation is synonymous with riskbenefit evaluation. |
Risk management is a decision-making process involving consideration of political, social, economic, and technical factors with relevant risk assessment information relating to a hazard to determine an appropriate course of action. |
Safety is the practical certainty that adverse effects will not result from exposure to a chemical substance under defined circumstances. It is the reciprocal of risk. |
Screening criteria are concentration values used in screening. Usually published for the purpose by an authoritative body (for example, HILs) or derived according to a specified methodology. Screening criteria are available for soil, groundwater, surface water and sediment. |
Screening is the process of comparison of site data to screening criteria to obtain a rapid assessment of contaminants of potential concern. |
Sensitive groups refers to sub-populations with both susceptibility and vulnerability factors. |
Sensitivity analysis is the process of changing one variable (input) while leaving the others constant and determining the effect on the output. The procedure involves fixing each uncertain quantity, one at a time, at its credible lower bound and then its upper bound (holding all other at their medians), and then computing the outcomes for each combination of values (US EPA 1992). It can be used to test the effects of both uncertainty and variability in input values. |
Site means the parcel of land being assessed for contamination. |
Site-specific target levels are risk-based concentration values derived using Tier 2 or Tier 3 exposure modelling. May be used as criteria for further assessment or as clean-up levels. |
Source is the contaminant that is considered to represent a potential risk requiring assessment. |
Subchronic exposure is contact between a chemical substance (agent) and a target of intermediate duration between acute and chronic. Different bodies vary on their definitions of the duration of ‘subchronic’ exposure, since it varies with species. US EPA uses up to 10% of an organism’s lifetime; however, between 36 months is often used when discussing subchronic exposure to people. |
Susceptibility refers to intrinsic biological factors that can increase the health risk of an individual at a given exposure level; examples of susceptibility factors include genetic factors, late-age and early-life, prior or existing disease. |
Threshold is the dose or exposure concentration of a chemical substance below which a stated effect is not observed or expected to occur. |
Tier 1 evaluation is a risk-based analysis comparing site data with generic published screening criteria for various land uses (for example, residential, commercial and industrial). This tier has the lowest data requirement, generic exposure assumptions, and applies the most conservative criteria. |
Tier 2 evaluation is a site-specific assessment in which risks to potentially exposed populations are assessed using site-specific data on pathways, land uses and the characteristics of the exposed populations. A Tier 2 evaluation usually involves the use of a quantitative exposure model. A Tier 2 evaluation is more complex than a Tier 1 evaluation and requires more site-specific information. As a result, a health protective effect will be achieved with a lower level of conservatism. |
Tier 3 evaluation is a further step from a Tier 2 evaluation and looks in more detail at specific risk-driving factors. This often involves additional data collection, and may incorporate more sophisticated modelling techniques. |
Tolerable daily intake (TDI) is analogous to acceptable daily intake. The term ‘tolerable’ is used for substances that are not deliberately added, such as contaminants in food and water. |
Toxicity is the inherent property of a chemical or material to cause an adverse biological effect. |
Toxicity reference value (TRV) is a measure of tolerable intake or acceptable risk. The TRV may be associated with either a threshold (i.e. ADI, TDI, TC or reference dose) or non-threshold (i.e. slope factor or unit risk) doseresponse relationship. |
Uncertainty analysis is a methodology that takes into account domain knowledge and its limitations in qualifying or quantifying (or both) the uncertainty in the structure of a scenario, structure of a model, inputs to a model and outputs of a model. |
Uncertainty is a lack or incompleteness of information or knowledge. In risk assessment, uncertainty has been defined by IPCS (2004) as ’imperfect knowledge concerning the present or future state of an organism, system, or population under consideration‘. |
Unit risk is the plausible upper-bound estimate of the probability of a response from a chemical over a lifetime expressed in units of concentration for a specified medium. |
Uptake is the amount of contaminant that enters the body through a barrier such as the skin, lungs or gut lining. Uptake is generally less than intake because not all the contaminant that enters the lungs or gut, or contacts the skin, is absorbed. |
Vadose zone is the portion of the sub-surface between the water table and the ground surface, also termed the unsaturated zone. Soil pore space in the vadose zone is only partially occupied by water, which is held in place by capillary forces and adhesion to soil particles. |
Variability describes true differences in attributes or values due to diversity or heterogeneity. |
Vulnerability refers to human populations at higher risk due to environmental factors. Examples of vulnerability factors include age, existing or past illness, poverty and other social determinants, smoking, poor nutrition, poor sanitation, behaviour more often associated with severe or profound intellectual disability (for example, pica).
|
ABS | Australian Bureau of Statistics |
ADI | acceptable daily intake |
ADWG | Australian Drinking Water Guidelines |
AM | arithmetic mean |
BaP | benzo(a)pyrene |
BMD | benchmark dose |
CCME | Canadian Council of Ministers of the Environment |
CF | concentration factor |
CRC CARE | Cooperative Research Centre for Contamination Assessment and Remediation of the Environment |
CSF | cancer slope factor |
CSIRO | Commonwealth Scientific and Industrial Research Organisation |
CSM | conceptual site model |
DAF | dermal absorption factor |
DDT | dichlorodiphenyltrichloroethane |
DEFRA | Department of Environment, Food and Rural Affairs (UK) |
DL | indoor dust loading factor |
DNA | deoxyribose nucleic acid |
DQO | data quality objective |
EA | Environment Agency (England and Wales) |
EHC | Environmental Health Criteria |
GAF | gastrointestinal absorption factor |
HEC | human equivalent concentration |
HED | human equivalent dose |
HI | hazard index |
HILs | health investigation levels |
HQ | hazard quotient |
HRA | health risk assessment |
HSL | health screening level |
IARC | International Agency for Research on Cancer |
IEUBK | US EPA integrated exposure uptake biokinetic model |
ILCR | increased lifetime cancer risk |
LOAEL | lowest observable adverse effect level |
LOEL | lowest observable effect level |
MF | modifying factor |
MfE | Ministry for Environment (NZ) |
MoA | mode (or mechanism) of action |
MRL | Minimal risk level |
NAPL | non-aqueous phase liquid |
NEPC | National Environment Protection Council |
NEPM | National Environment Protection Measure (1999) |
NHMRC | National Health and Medical Research Council |
NOAEL | no observable adverse effect level |
NOEL | no observable effect level |
PAHs | polycyclic aromatic hydrocarbons |
PBDE | polybrominated diphenyl ether |
PCBs | polychlorinated biphenyls |
PCDD | polychlorinated debenzo-p-dioxin |
PCDF | polychlorinated debenzofuran |
PCE | perchloroethylene (tetrachloroethene) |
PEF | particulate emission factor |
PM | particulate matter |
POP | persistent organic pollutant |
PTDI | provisional tolerable daily intake |
PTDI | provisional tolerable monthly intake |
PTWI | provisional tolerable weekly intake |
REL | reference exposure level |
RfC | reference concentration |
RfD | reference dose |
RI | risk index |
RQ | risk quotient |
SD | standard deviation |
SF | slope factor |
TC | tolerable concentration |
TCE | trichloroethene |
TDI | tolerable daily intake |
TEF | toxicity equivalence factor |
TEQ | toxicity equivalence quotient |
TF | indoor dust transport factor |
TPH | total petroleum hydrocarbons |
TPHCWG | Total Petroleum Hydrocarbon Criteria Working Group |
TRV | toxicity reference value |
UCL | upper confidence limit |
UF | uncertainty factor |
UR | unit risk |
US EPA | United States Environmental Protection Agency |
VOC | volatile organic compound |
VOCC | volatile organic chlorinated compound |
WAD | weak acid dissociable cyanide (method) |
WHO | World Health Organization |
[1] For example, a person with a pre-existing illness, or those with pica behaviour (i.e. a tendency to eat soil).