CONTENTS
List of Tables and Figures
Introduction
General
Structure of this Guide
Application of this Guide
Whole person impairment
Entitlements under the DRCA
Non-economic loss
Compensation payable
Interim and final assessments
Increase in degree of whole person impairment
Survival of claims
Principles of assessment
Impairment and non-economic loss
Employability and incapacity
Permanent impairment
Impairment tables
Gradations of impairment
Combined impairments
Double assessment
Fingers and toes
Exceptions to Division 1
Interim assessments
Likelihood of reduction in degree of impairment
Aggravation
Reference
Glossary
Division 1—Impairment
Chapter 1—Cardio-vascular system
Table 1.1 Assessments of symptomatic activity levels
Table 1.2 Peripheral vascular disease
Table 1.3 Varicose veins, deep venous thrombosis, oedema, ulceration
Chapter 2—Respiratory system
Table 2.1 Ventilatory function
Figure 2.1 Prediction nomogram—males
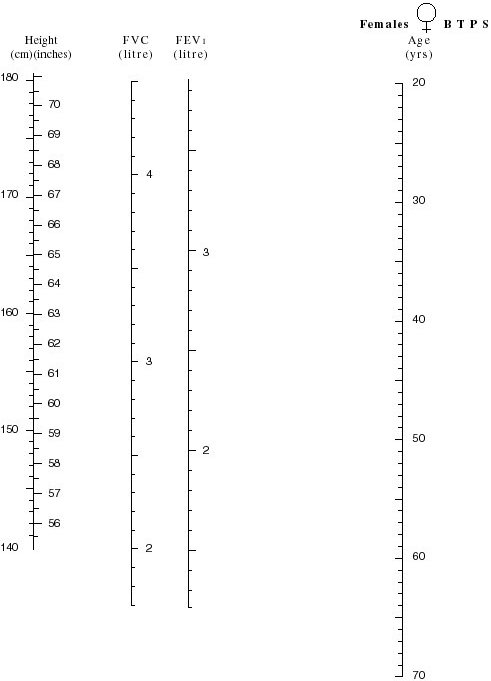
Figure 2.2 Prediction nomogram—females
Chapter 3—Endocrine system
Table 3.1 Endocrine system
Chapter 4—Skin disorders
Table 4.1 Functional loss
Table 4.2 Facial disfigurement
Chapter 5—Psychiatric conditions
Table 5.1 Psychiatric conditions
Chapter 6—Visual system
Table 6.1 Disorders of visual acuity
Chapter 7—Ear, nose and throat disorders
Table 7.1 Hearing
Table 7.2 Miscellaneous ear, nose and throat disorders
Chapter 8—Digestive system
Table 8.1 Disorders of the oesophagus, stomach, duodenum, small intestine, pancreas, colon, rectum and anus
Table 8.2 Disorders of the liver and biliary tract
Table 8.3 Fistulae and herniae
Chapter 9—Musculo-skeletal system
Table 9.1 Upper extremity
Table 9.2 Lower extremity
Table 9.3 Amputations and/or total loss of function
Table 9.4 Limb function—upper limb
Table 9.5 Limb function—lower limb
Table 9.6 Spine
Chapter 10—Urinary system
Table 10.1 Upper urinary tract
Table 10.2 Lower urinary tract
Chapter 11—Reproductive system
Table 11.1 Male
Table 11.2 Female
Table 11.3 Mammary glands
Chapter 12—Neurological function
Table 12.1 Cranial nerves
Table 12.2 Comprehension
Table 12.3 Expression
Table 12.4 Memory
Table 12.5 Reasoning
Chapter 13—Miscellaneous
Table 13.1 Intermittent conditions
Table 13.2 Malignancies
Chapter 14—Combined values chart
Table 14.1 Combined values chart
Division 2—Non-economic loss
B1 Pain and suffering
Table B1.1 Pain
Table B1.2 Suffering
B2 Loss of amenities
Table B2.1 Mobility
Table B2.2 Social relationships
Table B2.3 Recreation and leisure activities
B3 Other loss
Table B3 Other loss
B4 Loss of expectation of life
Table B4 Loss of expectation of life
B5 Calculation of non-economic loss
Table B5 Calculation of non-economic loss
Division 3—Calculation of the total entitlement to compensation for permanent impairment and non-economic loss
Worksheet C1 Calculation of total entitlement
Table 1.1 Assessments of symptomatic activity levels
Table 1.2 Peripheral vascular disease 19
Table 1.3 Varicose veins, deep venous thrombosis, oedema, ulceration 20
Table 2.1 Ventilatory function 21
Figure 2.1 Prediction nomogram—males 22
Figure 2.2 Prediction nomogram—females 23
Table 3.1 Endocrine system 24
Table 4.1 Functional loss 25
Table 4.2 Facial disfigurement 26
Table 5.1 Psychiatric conditions
Table 6.1 Disorders of visual acuity 29
Table 7.1 Hearing 30
Table 7.2 Miscellaneous ear, nose and throat disorders 30
Table 8.1 Disorders of the oesophagus, stomach, duodenum, small intestine, pancreas, colon, rectum and anus 31
Table 8.2 Disorders of the liver and biliary tract
Table 8.3 Fistulae and herniae
Table 9.1 Upper extremity
Table 9.2 Lower extremity 36
Table 9.3 Amputations and/or total loss of function 37
Table 9.4 Limb function—upper limb 38
Table 9.5 Limb function—lower limb 38
Table 9.6 Spine 39
Table 10.1 Upper urinary tract 40
Table 10.2 Lower urinary tract 41
Table 11.1 Male 42
Table 11.2 Female 43
Table 11.3 Mammary glands 43
Table 12.1 Cranial nerves 44
Table 12.2 Comprehension 46
Table 12.3 Expression 47
Table 12.4 Memory 48
Table 12.5 Reasoning 49
Table 13.1 Intermittent conditions 50
Table 13.2 Malignancies 51
Table 14.1 Combined values chart
Table B1.1 Pain 57
Table B1.2 Suffering 57
Table B2.1 Mobility 58
Table B2.2 Social relationships 59
Table B2.3 Recreation and leisure activities 59
Table B3 Other loss 60
Table B4 Loss of expectation of life 61
Table B5 Calculation of non-economic loss
Worksheet C1 Calculation of total entitlement
1 The Commonwealth Safety, Rehabilitation and Compensation (Defence-Related Claims) Act 1988 (also referred to as the “DRCA”) provides for payment of lump sum compensation for permanent impairment and non-economic loss resulting from injuries suffered by members of the Defence Force while engaged in defence service before 1 July 2004.
Note 1: The DRCA refers to members (and former members) of the Defence Force who may be eligible for compensation under that Act as employees (see section 5 of that Act). The term “employee” is also used in this Guide to refer to such members and former members.
Note 2: Compensation for injuries suffered by members of the Defence Force while engaged in defence service on or after 1 July 2004 is assessed under the Military Rehabilitation and Compensation Act 2004.
Note 3: Compensation for such injuries that became permanent before 1 December 1988 is assessed under the Compensation (Commonwealth Government Employees) Act 1971.
2 The amount of compensation payable is to be assessed by reference to the degree of permanent impairment and the degree of non-economic loss determined by the MRCC under this Guide.
Note: For the compensation payable, see sections 24 to 28 of the DRCA. For the scope of defence service concerned, see section 4AA of that Act.
3 Division 1 is used to assess the degree of the permanent impairment of an employee resulting from an injury. Table 14.1 (Combined values chart) is used to obtain the combined value of multiple impairments resulting from a single injury where combination is required.
4 Division 2 is used to assess the degree of non-economic loss suffered by an employee as a result of an injury or impairment.
5 Division 3 is used to calculate the total entitlement to compensation for permanent impairment and non-economic loss, based on the assessments completed in Divisions 1 and 2.
6 The Principles of assessment and Glossary contain information relevant to the interpretation and application of Divisions 1, 2 and 3.
7 This Guide applies to the assessment or re-assessment of the degree of permanent impairment of an employee resulting from an injury, or the degree of non-economic loss suffered by an employee as a result of an injury or impairment, relating to a claim for compensation under section 24, subsection 25(4) or (5) or section 27 of the DRCA if the claim is received by the relevant authority on or after the day this instrument commences (the commencement day).
8 This Guide applies to a re-assessment mentioned in paragraph 7 in relation to a claim received before the commencement day if the request for re-assessment is received on or after the commencement day.
9 This Guide applies in relation to:
(a) a reconsideration of a determination under section 62 of the DRCA that relates to an assessment or re-assessment to which paragraph 7 or 8 of this Guide applies; and
(b) a review by the Administrative Appeals Tribunal of a decision under subsection 38(4) (review of certain determinations by the MRCC) or section 62 (reconsideration of determinations) of the DRCA that relates to an assessment or re-assessment to which paragraph 7 or 8 of this Guide applies.
10 Despite the repeal of the Safety, Rehabilitation and Compensation Act 1988—Guide to the Assessment of the Degree of Permanent Impairment Edition 2.1 [F2012C00537], any relevant earlier Guide in force immediately before the commencement day continues in force after the commencement day, subject to paragraphs 7, 8 and 9 of this Guide, for the following purposes:
(a) determining a claim made before the commencement day under the DRCA; and
(b) an interim determination and assessment under subsection 25(1) of the DRCA in relation to such a claim.
Note 1: The repealed Guide mentioned in this subsection is repealed by the Safety, Rehabilitation and Compensation Act 1988—Guide to the Assessment of the Degree of Permanent Impairment Edition 3.0.
Note 2: Part 2 of the repealed Guide (and of previous editions of that Guide) applied to the determination of claims under the DRCA.
11 Each of the following is a relevant earlier Guide for a claim mentioned in paragraph 10:
(a) the repealed Guide mentioned in that paragraph;
(b) any previous edition of that Guide that applied in relation to the claim immediately before the commencement day.
12 Prior to 1988, the Compensation (Commonwealth Government Employees) Act 1971 (repealed with the coming into effect of the SRC Act and (in 2017) the DRCA) provided for the payment of lump sum compensation where an employee suffered the loss of, or loss of efficient use of, a part of the body or faculty, as specified in a table of maims. The range of conditions compensated was exclusive and did not reflect the broad range of work-related conditions.
13 Whole person impairment (also referred to as “WPI”) is the methodology used in this Guide (and in previous editions of this Guide) for expressing the degree of impairment of a person, resulting from an injury, as a percentage. The concept of WPI is drawn from the AMA Guides (where it is referred to as “whole man” impairment).
14 Subsection 24(5) of the DRCA provides for the determination of the degree of permanent impairment of the employee resulting from an injury, that is, the employee as a whole person. The whole person impairment concept, therefore, provides for compensation for the permanent impairment of any body part, system or function to the extent to which it permanently impairs the employee as a whole person.
15 Paragraph 28(1)(a) of the DRCA provides for the Guide to set out criteria by reference to which the degree of the permanent impairment of an employee resulting from an injury shall be determined. Paragraph 28(1)(c) of the DRCA relevantly provides that methods by which the degree of permanent impairment, as determined under those criteria, shall be expressed as a percentage. Subsection 28(5) of the DRCA relevantly provides that the percentage of permanent impairment suffered by an employee as a result of an injury ascertained under the methods referred to in paragraph 28(1)(c) of that Act may be 0%.
16 Whole person impairment is the methodology used in this Guide in accordance with section 28 of the DRCA and is therefore the methodology by which the degree of permanent impairment of an employee resulting from an injury is expressed as a percentage. While the employee’s impairment resulting from a particular injury is to be assessed against criteria in this Guide by reference to the functional capacities of a normal healthy person, the degree of permanent impairment of that employee resulting from that particular injury may be assessed as:
(a) 0% if there is no increase in the employee’s whole person impairment when assessed in accordance with this Guide; or
(b) less than the threshold for compensation under section 24 of the DRCA even if there is an increase in the employee’s whole person impairment when assessed in accordance with this Guide.
17 Where the degree of permanent impairment of the employee (other than a hearing loss) is determined by the relevant authority under subsection 24(5) of the DRCA to be less than 10%, subsection 24(7) of that Act provides that compensation is not payable to the employee under section 24 of that Act.
18 Subsection 24(8) of the DRCA excludes the operation of subsection 24(7) in relation to impairment constituted by the loss, or the loss of the use, of a finger or toe, or the loss of the sense of taste or smell. The threshold for compensation under section 24 of the DRCA for an injury resulting in a permanent impairment constituted by such a loss is 1% to 5% WPI under this Guide depending on the nature of the impairment.
19 For injuries suffered by employees after 1 October 2001, subsection 24(7A) of the DRCA provides, in effect, that, if the injury results in a permanent impairment that is a hearing loss, the 10% threshold does not apply. In those cases:
(a) subsection 24(7A) of the DRCA provides that compensation is not payable to the employee under section 24 if the relevant authority determines the binaural hearing loss suffered by the employee to be less than 5%; and
(b) Table 7.1 (Hearing) provides that the percentage of binaural hearing loss is converted to a WPI rating by dividing the percentage of binaural hearing loss by 2; and
(c) consequently, the threshold for compensation under section 24 of the DRCA for an injury resulting in a permanent impairment that is a hearing loss is 2.5% WPI under this Guide.
20 Subsection 27(1) of the DRCA provides that where there is liability to pay compensation in respect of a permanent impairment, additional compensation for non-economic loss is payable in accordance with section 27 of that Act.
21 Non-economic loss is assessed under Division 2 of this Guide.
22 The maximum level of payment is prescribed in subsection 24(9) of the DRCA, and indexed annually on 1 July in accordance with the Consumer Price Index under section 13 of that Act. Compensation is calculated at the rate applicable at the time of the assessment. See Division 3 of this Guide for calculation of total entitlements to compensation for permanent impairment and non-economic loss.
23 On the written request of the employee under subsection 25(1) of the DRCA, an interim determination must be made by the relevant authority of the degree of permanent impairment suffered and an assessment made of an amount of compensation payable to the employee, where:
(a) a determination has been made that an employee has suffered a permanent impairment as a result of an injury; and
(b) the degree of that impairment is equal to or more than 10%; and
(c) a final determination of the degree of permanent impairment has not been made.
24 When a final determination of the degree of permanent impairment is made by the relevant authority, there is payable to the employee, under subsection 25(3) of the DRCA, an amount equal to the difference, if any, between the final determination and the interim assessment.
25 Where a final assessment of the degree of permanent impairment has been made by the relevant authority and the level of whole person permanent impairment subsequently increases by 10% or more in respect of the same injury, the employee may request, pursuant to subsection 25(4) of the DRCA, another assessment for compensation for permanent impairment and non-economic loss. Additional compensation is payable for the increased level of whole person impairment only.
26 For injuries suffered by employees after 1 October 2001, pursuant to subsection 25(5) of the DRCA, if the injury results in a permanent impairment that is a hearing loss, there may be a further amount of compensation payable if there is a subsequent increase in the binaural hearing loss of 5% or more. In those cases:
(a) Table 7.1 (Hearing) provides that the percentage of binaural hearing loss is converted to a WPI rating by dividing the percentage of binaural hearing loss by 2; and
(b) consequently, the threshold for additional compensation under section 25 of the DRCA for an injury resulting in a permanent impairment that is a hearing loss is 2.5% WPI under this Guide.
Note: See Application of this Guide for assessments and re-assessments of the degree of permanent impairment made under relevant earlier editions of this Guide.
27 The DRCA provides for the survival of certain claims for compensation. If an employee suffers an injury resulting in permanent impairment, and the employee dies:
(a) before a claim for permanent impairment compensation has been made—the employee’s personal representative may make such a claim (see subsections 4(11) and 55(1) of the DRCA); or
(b) after a claim for permanent impairment compensation has been made—the employee’s personal representative may continue with the claim (see subsections 4(11) and 55(2) of the DRCA).
28 In either case mentioned in subsection (1), if an amount of compensation is determined by the relevant authority to be payable under section 24 of the DRCA in respect of the claim, subject to section 111 of that Act, the amount is payable to the deceased employee’s estate (see subsections 55(3) and 111(1) of that Act). No compensation under section 27 of the DRCA would be payable to the deceased employee’s estate for any non-economic loss (see subsection 55(4) of that Act).
29 Impairment is defined by the DRCA as the “loss, the loss of the use, or the damage or malfunction, of any part of the body or of any bodily system or function or part of such system or function” (see subsection 4(1) of that Act).
Note: For the assessment of the degree of impairment, see Division 1.
30 Impairment relates to the health status of an individual and includes anatomical loss, anatomical abnormality, physiological abnormality and psychological abnormality.
31 In this Guide, loss of function is used as a basis of assessment of impairment and as far as possible objective criteria have been used. The degree of impairment is assessed by reference to the impact of that loss by reference to the functional capacities of a normal healthy person.
32 Impairment is measured against its effect on personal efficiency in the activities of daily living in comparison with a normal healthy person.
Note: Activities of daily living are defined in the Glossary.
33 Non-economic loss is defined by the DRCA, in relation to an employee who has suffered an injury resulting in a permanent impairment, as “loss or damage of a non‑economic kind suffered by the employee (including pain and suffering, a loss of expectation of life or a loss of the amenities or enjoyment of life) as a result of that injury or impairment and of which the employee is aware.” (see subsection 4(1) of that Act).
Note: For the assessment of the degree of non-economic loss, see Division 2.
34 Non-economic loss is a subjective concept of the effects of the impairment on the employee’s life. It includes loss of expectation of life and any other real inconveniences caused by the impairment.
35 Whilst activities of daily living are used to assess impairment they should not be confused with “lifestyle effects” which are used to assess non-economic loss. Lifestyle effects are a measure of an individual’s mobility and enjoyment of, and participation in, recreation, leisure activities and social relationships.
36 It is emphasised that the employee must be aware of the non-economic losses suffered. While employees may have equal ratings of impairment it would not be unusual for them to receive different ratings for non-economic loss because of their different lifestyles.
37 The concepts of “employability” and “incapacity” are not included in the assessment of impairment and non-economic loss. Incapacity is influenced by factors other than the degree of impairment and is compensated by weekly payments which are in addition to these payments.
38 Compensation is only payable for an impairment resulting from an injury which is permanent. In the DRCA, “permanent” means “likely to continue indefinitely” (see subsection 4(1) of that Act).
39 For the purpose of determining whether an impairment is permanent under the DRCA, the assessor must have regard to all of the matters in subsection 24(2) of that Act, namely the following:
(a) the duration of the impairment;
(b) the likelihood of improvement in the employee’s condition;
(c) whether the employee has undertaken all reasonable rehabilitative treatment for the impairment;
(d) any other relevant matters.
40 An impairment will generally be regarded as permanent when the recovery process has been completed, that is, when the full and final effects of convalescence, the natural healing process and active (as opposed to palliative) medical treatment have been achieved.
41 The impairment tables in Division 1 are based on the concept of “whole person impairment”, which is drawn from the AMA Guides.
42 Evaluation of whole person impairment is a medical appraisal of the nature and extent of the effect of an injury or disease on a person’s functional capacity and activities of daily living.
43 As with the AMA Guides, Division 1 is structured by assembling detailed descriptions of impairments into groups according to body system and expressing the extent of each impairment as a percentage value of the functional capacity of a normal healthy person. Thus a percentage value can be assigned to an employee’s impairment by reference to the relevant description in this Guide.
44 Each table in Division 1 contains impairment values at gradations of 5% or multiples of 5%. Where it is not clear which of 2 impairment values is more appropriate, the relevant authority has the discretion to determine which value properly reflects the degree of impairment.
45 There is no discretion to choose an impairment value not specified in Division 1. For example, where 10% and 20% are specified values there is no discretion to determine impairment as 15%.
46 Where a table in Division 1 provides for impairment values within a range, consideration will need to be given to all criteria applicable to the condition, which includes performing activities of daily living and an estimate of the degree to which the medical impairment interferes with these activities.
47 In some cases, additional information may be required to determine where to place an individual within the range. The person conducting the assessment must provide written reasons why the person considers the selected point within the range as clinically justifiable.
48 Impairment is system or function based. A single injury may give rise to multiple loss of function. When more than one table in Division 1 applies to a single injury, separate scores should be allocated to each functional impairment.
Note: The scores are then combined using Table 14.1 (Combined values chart). See also Double assessment.
49 Where there is an initial injury which results in impairment, and a second injury which results in impairment to the same bodily system or function occurs, the pre-existing impairment must be disregarded when assessing the degree of impairment of the second injury. The second injury should be assessed by reference to the functional capacities of a normal healthy person.
50 The possibility of double assessment for a single loss of function must be guarded against. For example, it would be inappropriate to assess a lower limb amputation by reference to both Table 9.3 (Amputations and/or total loss of function) and Table 9.2 (Lower extremity).
51 Where an employee suffers from more than one impairment arising from the same injury (see Combined impairments (multiple impairments)), the values are not added but are combined using Table 14.1 (Combined values chart).
52 The purpose of Table 14.1 (Combined values chart) is to give the total effect of all impairments, according to a formula, as a percentage value of the employee’s whole bodily system or function.
53 Impairment relating to the loss or injury to a finger or toe refers not only to amputation or total loss of efficient use of the whole digit, but also to partial loss of efficient use of a digit.
54 In the event that an impairment is of a kind that cannot be assessed in accordance with the provisions of Division 1, the relevant authority may direct that the assessment be made in accordance with the AMA5, and the assessment must accordingly be so made.
55 To ensure that the possibility of entitlement to a permanent impairment payment does not impede the rehabilitation process, provision is made under subsection 25(1) of the DRCA for interim assessment and payment of compensation.
56 Assessment for an interim payment will apply mainly in cases undergoing active treatment where the final outcome of the treatment is not known but a minimum permanent impairment can be measured.
57 Care should be taken to ensure that further treatment will not reduce the impairment, which must be at least 10%.
58 Interim payment will generally not apply where the impairment has stabilised or where the only change in impairment would be due to progressive degeneration.
59 The relevant authority must have regard to medical opinion concerning the nature and effect (including possible effect) of the injury and the extent (if any) to which impairment resulting from the injury or non-economic loss resulting from the injury or impairment, may reasonably be capable of being reduced or removed.
60 In particular, regard must be had to an employee’s unreasonable failure or refusal to act in accordance with medical advice or to submit to medical treatment which would reduce the degree of impairment.
61 A permanent impairment assessment in respect of an aggravation should not be made unless the effects of an aggravation are considered permanent. If the employee’s impairment is entirely attributable to a pre-existing or underlying condition, or to the natural progression of such a condition, the assessment for permanent impairment should be nil.
62 Where it is possible to isolate the compensable effects of an injury upon a pre-existing or underlying condition the assessment of the degree of permanent impairment should reflect only the impairment due to those compensable effects.
63 American Medical Association, 2001, Guides to the Evaluation of Permanent Impairment, 5th edition, Chicago: American Medical Association.
Note: This is referred to as AMA5 (see the Glossary to this Guide).
Note 1: An expression used in this Guide has the same meaning as in the DRCA, unless the contrary intention appears: see paragraph 13(1)(b) of the Legislation Act 2003.
Note 2: A number of expressions used in this Guide are defined in the DRCA, including the following (references are to the DRCA):
(a) aggravation (subsection 4(1));
(b) ailment (subsection 4(1));
(c) claim (subsection 4(1));
(d) employee (section 5);
(e) impairment (subsection 4(1));
(f) injury (subsections 4(3) and (8) and sections 5A, 123A and 124);
(g) MRCC (short for Military Repatriation and Compensation Commission) (subsection 4(1));
(h) non-economic loss (subsection 4(1));
(i) permanent (subsection 4(1));
(j) relevant authority (subsection 4(1));
(k) SRC Act (short for Safety, Rehabilitation and Compensation Act 1988) (subsection 4(1)).
In this Guide:
activities of daily living means the activities a person needs to perform to function in a non-specific environment (that is, to live). The measure of activities of daily living is a measure of primary biological and psychosocial function. These activities are as follows:
(a) the ability to receive and to respond to incoming stimuli;
(b) standing;
(c) moving;
(d) feeding (including eating, but not including the preparation of food);
(e) control of bladder and bowel;
(f) self-care (for example, bathing and dressing);
(g) sexual function.
AMA2 means the American Medical Association, 1984, Guides to the Evaluation of Permanent Impairment, 2nd edition, Chicago: American Medical Association, and any errata published prior to the commencement day.
AMA5 means the American Medical Association, 2001, Guides to the Evaluation of Permanent Impairment, 5th edition, Chicago: American Medical Association, and any errata published prior to the commencement day.
AMA Guides means the American Medical Association, Guides to the Evaluation of Permanent Impairment (Chicago: American Medical Association) (various editions).
commencement day: see Application of this Guide.
disease has its ordinary meaning.
DRCA means the Safety, Rehabilitation and Compensation (Defence-related Claims) Act 1988.
loss of amenities, in relation to an employee, means effects on the employee’s mobility, social relationships and recreation and leisure activities.
%NEL means percentage of non-economic loss.
pain means physical pain.
re-assessment means a re-assessment of the degree of permanent impairment for the purposes of subsection 25(4) or (5) of the DRCA (interim payment of compensation).
suffering means mental distress resulting from the impairment or injury.
Examples: Grief, anguish, fear, frustration, humiliation, embarrassment, etc.
whole person impairment: see the Introduction and the Principles of assessment.
WPI is short for whole person impairment.
%WPI means percentage of whole person impairment.
Table of metabolic costs of activities will be provided for purposes of assessment. Examples of conditions with which it can be used are ischaemic heart disease, rheumatic heart disease and hypertension.
Male Symptomatic level of activity in METs
(%WPI) |
AGE
(Yrs) | 1 | 1-2 | 2-3 | 3-4 | 4-5 | 5-6 | 6-7 | 7-8 | 8-9 | 10+ |
18-30 | 95 | 80 | 70 | 60 | 50 | 45 | 35 | 25 | 10 | 5 |
31-40 | 95 | 80 | 70 | 60 | 50 | 40 | 30 | 15 | 5 | - |
41-50 | 95 | 75 | 65 | 50 | 40 | 25 | 15 | 5 | - | - |
51-60 | 95 | 75 | 60 | 45 | 30 | 15 | 10 | 5 | - | - |
61-70 | 95 | 70 | 55 | 40 | 25 | 10 | 5 | - | - | - |
70+ | 95 | 65 | 45 | 30 | 10 | - | - | - | - | - |
Female Symptomatic level of activity in METs
(%WPI) |
AGE
(Yrs) | 1 | 1-2 | 2-3 | 3-4 | 4-5 | 5-6 | 6-7 | 7-8 | 8-9 | 10+ |
18-30 | 95 | 80 | 65 | 60 | 40 | 25 | 15 | 10 | 5 | - |
31-40 | 95 | 80 | 60 | 45 | 35 | 20 | 5 | - | - | - |
41-50 | 95 | 75 | 60 | 45 | 30 | 15 | 5 | - | - | - |
51-60 | 95 | 75 | 55 | 35 | 20 | 10 | 5 | - | - | - |
61-70 | 95 | 70 | 45 | 30 | 10 | 5 | - | - | - | - |
70+ | 95 | 65 | 30 | 15 | 5 | - | - | - | - | - |
% WPI | Description of level of impairment |
0 | The claimant experiences neither intermittent claudication nor ischaemic pain at rest. |
5 | The claimant has no difficulty with distances but experiences ischaemic pain on climbing steps or gradients. |
10 | The claimant experiences claudication on walking 200 metres or more at an average walking pace on level ground. |
20 | The claimant experienced claudication on walking more than 100 but less than 200 metres at average pace on level ground. |
30 | The claimant experiences claudication on walking more than 75 but less than 100 metres at average pace on level ground. |
40 | The claimant experiences claudication on walking more than 50 but less than 75 metres at average pace on level ground. |
50 | The claimant experiences claudication on walking more than 25 but less than 50 metres at average pace on level ground. |
60 | The claimant experiences claudication on walking less than 25 metres at average pace on level ground. |
70 | The claimant experiences ischaemic pain at rest. |
% WPI | Description of level of impairment |
0 | One or more of the following: - varicose veins—may be gross but cause no significant restriction of activities
- oedema—mild or transient
- skin reaction—mild or transient
and minimal limitation of activities of daily living (although exacerbation may temporarily increase the extent of limitation). |
10 | Any one of the following which necessitates intermittent treatment including a short period of admission to hospital or confinement to home: - varicose veins—with recurrent superficial phlebitis
- oedema—persistent and incompletely controlled
- ulceration—superficial, transient.
|
15 | Any two of the following which necessitate intermittent treatment including a short period of admission to hospital or confinement to home: - varicose veins—with recurrent superficial phlebitis
- oedema—persistent and incompletely controlled
- ulceration—superficial, transient.
|
20 | All of the following which necessitate intermittent treatment including a short period of admission to hospital or confinement to home: - varicose veins—with recurrent superficial phlebitis
- oedema—persistent and incompletely controlled
- ulceration—superficial, transient.
|
30 | Any one of the following which needs continuous treatment including periodic admission to hospital or confinement to residence: - deep venous thrombosis
- oedema—marked and only partly controlled by elastic support or medication
- ulceration—persistent, widespread or deep.
|
40 | Any two of the following which need continuous treatment including periodic admission to hospital or confinement to residence: - deep venous thrombosis
- oedema—marked and only partly controlled by elastic support or medication
- ulceration—persistent, widespread or deep.
|
50 | Severe bilateral deep venous thrombosis which needs continuous treatment including long periods of admission to hospital or confinement to residence. |
60 | Any two of the following which need continuous treatment including long periods of admission to hospital or confinement to residence: - severe bilateral deep venous thrombosis
- marked oedema that cannot be controlled
- severe ulceration.
|
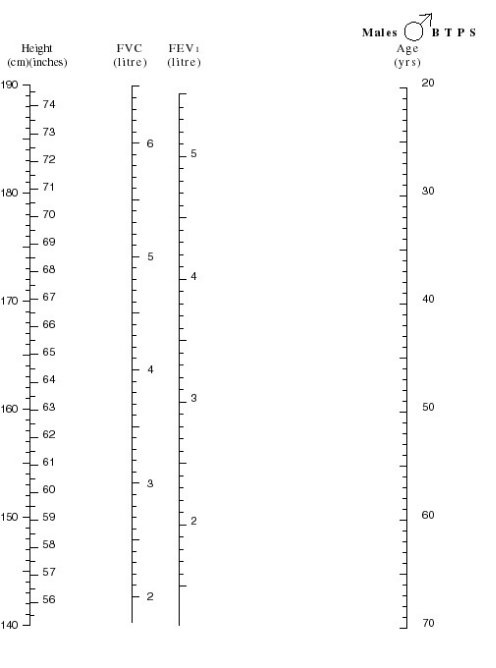
The major test of respiratory impairment is the ventilatory function test or respiratory test. Predictive nomograms for the forced expiratory volume over one second (FEV1) and the forced vital capacity (FVC) are at Figures 2.1 (males) and 2.2 (females).
% WPI | Ventilatory function %
of predicted value |
0 | More than 85 |
10 | 85 |
15 | 80 |
20 | 75 |
25 | 70 |
30 | 65 |
35 | 60 |
40 | 55 |
45 | 50 |
50 | 45 |
55 | 40 |
60 | 35 |
65 | 30 |
70 | 25 |
Notes
- X-rays may be normal in any of the above categories.
- Measurement of FEV1 and Forced Vital Capacity (FVC) should be performed with a Vitalograph® spirometer or equivalent instrument.
- Three readings should be taken and the largest of these used to calculate impairment.
The effects of diabetes mellitus in other systems (for example, the vascular and visual systems) should be assessed from the appropriate tables and combined with values from the table above using Table 14.1 (Combined values chart).
% WPI | Description of level of impairment |
0 | Any one of the following: - thyroid disease adequately controlled with thyroxine replacement
- primary hyperparathyroidism; parathyroid adenoma removed; replacement therapy not indicated
- asymptomatic Paget’s disease
- asymptomatic osteoporosis or other bone disease, with or without treatment.
|
5 | Diabetes mellitus satisfactorily controlled by diet and/or oral medication. |
10 | Any one of the following: - thyroid disease which cannot be adequately treated with thyroxine
- primary hyperparathyroidism; parathyroidectomy; replacement therapy required
- symptomatic Paget’s disease
- symptomatic osteoporosis
- other bone disease WITH pain not completely controlled by continuous therapy.
|
15 | Diabetes mellitus requiring dietary adjustment and insulin. |
20 | Diabetes mellitus not satisfactorily controlled despite vigorous therapy. |
In the evaluation of impairment resulting from a skin disorder the actual functional loss is the prime consideration, rather than the extent of cutaneous involvement. Where the condition affects the face Table 4.2 (Facial disfigurement) may be more appropriate.
% WPI | Description of level of impairment |
0 | The condition is absent on examination or if present can easily be reversed by appropriate medication or other treatment and causes no interference with activities of daily living when present. |
5 | The condition requires treatment for lengthy periods but causes no interference with activities of daily living when present. |
10 | The condition is absent on examination or if present can easily be reversed by appropriate medication or treatment and causes minor interference with activities of daily living when present. |
20 | The condition requires treatment for periods in aggregate up to three months per year and causes interference with activities of daily living when present. |
30 | The condition requires treatment for periods in aggregate up to four months per year and causes minor interference with activities of daily living when present. |
40 | The condition requires treatment for periods in aggregate up to four months per year and causes major interference with activities of daily living when present. |
45 | The condition requires treatment for periods in aggregate up to six months per year and causes minor interference with activities of daily living when present. |
50 | The condition requires treatment for periods in aggregate up to six months per year and causes major interference with activities of daily living when present. |
60 | The condition requires treatment for periods in aggregate up to nine months per year and causes minor interference with activities of daily living when present. |
70 | The condition requires treatment for periods in aggregate up to nine months per year and causes major interference with activities of daily living when present. |
75 to 100 | The condition is present all the time and requires treatment for between 9 and 12 months of the year and causes major interference with activities of daily living. |
Note
- Assessors should refer to Gradations of impairment in the Principles of assessment for guidance on awarding an impairment value within a range.
When evaluating impairment due to facial injury or disease, three factors need to be considered:
- First, the functional components of the face must be evaluated (for example the effects of the condition on communication, respiration, eating, visual function, hearing, etc.).
- Second, the cosmetic effects should be considered. These are not truly an impairment, but for the purposes of evaluation are deemed to be equivalent to certain impairments. These deemed values are set out below. Cosmetic defects should be assessed when all feasible cosmetic surgery has been completed and should take into account the beneficial effects of the use of cosmetics etc.
- Third, facial disfigurement may result in behavioural changes. These should be assessed in accordance with the criteria in Table 5.1 (Psychiatric conditions).
- Where more than one deformity is present from the same band or different bands, a value should be allotted to each and these should be combined using Table 14.1 (Combined values chart).
% WPI | Description of level of impairment |
0 | Normal facial appearance or any scarring above the brow line. |
5 | Any of the following: - cutaneous scars or pigmentation
- unilateral facial paralysis
- distortion of the nose
- loss or deformity of the external ear.
|
10 | Any of the following: - disfigurement of the orbit
- bilateral facial paralysis
- depression of the zygoma
- depression of the frontal bones
- severe scarring below the upper lip.
|
15 | Loss of part of nose. |
25 | Loss of the entire nose. |
35 | Severe disfigurement of the entire area between the brow and the upper lip on both sides. |
Includes psychoses, neuroses, personality disorders and other diagnosable conditions. The assessment should be made on optimum medication at a stage where the condition is reasonably stable.
% WPI | Description of level of impairment |
0 | Reactions to stresses of daily living WITHOUT loss of personal or social efficiency AND retained capability of performing activities of daily living without supervision or assistance. |
5 | Despite the presence of ONE of the following, employee is capable of performing activities of daily living without supervision or assistance: - reactions to stresses of daily living with minor loss of personal or social efficiency
- lack of conscience-directed behaviour without harm to others or self
- minor distortion of thinking.
|
10 | Despite the presence of more than one of the following, employee is capable of performing activities of daily living without supervision or assistance: - reactions to stresses of daily living with minor loss of personal or social efficiency
- lack of conscience-directed behaviour without harm to others or self
- minor distortion of thinking.
|
15 | Any of the following, accompanied by a need for some supervision and direction in activities of daily living: - reactions to stresses of daily living which cause modification of daily living patterns
- marked disturbances in thinking
- definite disturbance in behaviour.
|
20 | Any two of the following, accompanied by a need for some supervision and direction in activities of daily living: - reactions to stresses of daily living which cause modification of daily living patterns
- marked disturbance in thinking
- definite disturbance in behaviour.
|
25 | All of the following, accompanied by a need for some supervision and direction in activities of daily living: - reactions to stresses of daily living which cause modification of daily living patterns
- marked disturbances in thinking
- definite disturbances in behaviour.
|
30 | Any one of the following, accompanied by a need for supervision and direction in activities of daily living: - hospital dischargees who require daily medication or regular therapy to avoid readmission
- loss of self control and/or inability to learn from experience causing considerable damage to self or others.
|
40 | Both of the following, accompanied by a need for supervision and direction in activities of daily living: - hospital dischargees who require daily medication or regular therapy to avoid readmission
- loss of self control and/or inability to learn from experience causing considerable damage to self or others.
|
50 | One of the following: - severe disturbances of thinking and/or behaviour which entails potential or actual harm to self and/or others
- need for supervision and direction in a confined environment.
|
60 | Both of the following - severe disturbances of thinking and/or behaviour which entails potential or actual harm to self and/or others
- need for supervision and direction in a confined environment.
|
90 | Very severe disturbance in all aspects of thinking and behaviour such as to require constant supervision and care in a confined environment and assistance with all activities of daily living. |
| | |
Disorders such as nystagmus, conjunctivitis, impaired colour vision, night blindness and glaucoma (without visual loss) are usually binocular and cause minimal impairment. An assessment of 0 to 5% is appropriate for such conditions.
Visual field defects should be accurately mapped and assessed in accordance with the procedures dictated in AMA2.
Impairment is based on corrected visual acuity.
Right eye |
L
e
f
t
e
y
e | % WPI
| 6/6 | 6/9 | 6/12 | 6/18 | 6/24 | 6/30 | 6/36 | 6/48 | 6/60 | 3/60 | No perceived light |
6/6 | 0 | 5 | 5 | 10 | 10 | 15 | 15 | 20 | 20 | 20 | 25 |
6/9 | 5 | 10 | 10 | 15 | 15 | 20 | 20 | 25 | 25 | 30 | 30 |
6/12 | 5 | 10 | 20 | 20 | 25 | 25 | 30 | 30 | 35 | 35 | 40 |
6/18 | 10 | 15 | 20 | 30 | 30 | 35 | 35 | 40 | 40 | 40 | 45 |
6/24 | 10 | 15 | 25 | 30 | 40 | 40 | 40 | 45 | 45 | 50 | 50 |
6/30 | 15 | 20 | 25 | 35 | 40 | 45 | 50 | 50 | 55 | 55 | 60 |
6/36 | 15 | 20 | 30 | 35 | 40 | 50 | 55 | 60 | 60 | 65 | 65 |
6/48 | 20 | 25 | 30 | 40 | 45 | 50 | 60 | 65 | 70 | 70 | 75 |
6/60 | 20 | 25 | 35 | 40 | 45 | 55 | 60 | 70 | 75 | 80 | 80 |
3/60 | 20 | 30 | 35 | 40 | 50 | 55 | 65 | 70 | 80 | 85 | 85 |
No perceived light | 25 | 30 | 40 | 45 | 50 | 60 | 65 | 75 | 80 | 85 | 85 |
Hearing defects are assessed in accordance with the current procedures from Australian Hearing Services (Hearing Australia).
Once the binaural percentage loss of hearing has been calculated, it is then converted to a WPI value.
The calculation for converting the percentage loss of hearing to a WPI rating is:

%
WPI | Description of level of impairment |
0 | One or more of the following: - intermittent otorrhoea
- intermittent otalgia and tinnitus
- post nasal discharge, rhinorrhoea and sneezing
- vertigo which does not interfere with any activities
- other conditions which are controlled by medication or for which no medication is required.
|
5 | Any of the following: - permanent otorrhoea
- complete loss of olfaction or taste
- permanent tinnitus.
|
10 | Any of the following: - permanent otalgia
- vertigo which interferes only with activities involving personal or public safety (for example, driving a car, operating machinery).
|
20 | Vertigo which interferes with activities of daily living. |
25 | Permanent tracheostomy or stoma. |
40 | Vertigo which interferes with all activities except household duties and self-care. |
60 | Vertigo which interferes with all activities to the extent that only self-care can be managed and all other activity is impossible. |
80 | Vertigo such that the sufferer is confined to home and requires assistance with all activities, including self-care. |
% WPI | Description of level of impairment |
0 | Symptoms present but no anatomical loss or alteration. |
5 | Symptoms and/or signs present and there is anatomical loss or alteration but continuous treatment is not required and weight and nutrition are maintained at normal levels or mild incontinence of flatus or liquid stool. |
10 | Objective signs of disease present and at least one of the following: - dietary modification needed for control
- drugs needed for control
- loss of up to 10% of desirable weight per range on standard BMI chart.
|
15 | Objective signs of disease present and at least two of the following: - dietary modification needed for control
- drugs needed for control
- loss of up to 10% of desirable weight per range on standard BMI chart.
|
20 | Partial faecal incontinence requiring continual treatment or objective signs of disease present and all of the following: - dietary modification needed for control
- drugs needed for control
- loss of up to 10% of desirable weight per range on standard BMI chart.
|
25 | Objective signs of disease present and one of the following: - dietary modification and drugs produce partial but incomplete control
- loss of 10% to 20% of desirable weight per range on standard BMI chart.
|
30 | Objective signs of disease present and both of the following: - dietary modification and drugs produce partial but incomplete control
- weight loss of 10% to 20% of desirable weight per range on standard BMI chart.
|
40 | Objective signs of disease present with two of the following: disturbed bowel habit pain (periodic or continual) continual manifestations (for example, fever or anaemia) weight loss of 10% to 20% of desirable weight per range on standard BMI chart. |
45 | Complete faecal incontinence |
50 | Objective signs of disease present with all of the following: - disturbed bowel habit
- pain (periodic or continual)
- continual manifestations (for example, fever or anaemia)
- weight loss of 10% to 20% of desirable weight per range on standard BMI chart.
|
55-75 | Objective signs of disease present and a combination of the following: - severe persistent disturbance of bowel habit
- severe persistent pain
- constitutional manifestations
- weight loss of more than 20% of desirable weight per range on standard BMI chart
- severe limitation of activity.
|
Note
% WPI | Description of level of impairment |
0 | Mildly abnormal liver function tests but adequate nutrition and strength with no other signs of disease. |
5 | Episodes of biliary colic twice a year or less frequently. |
10 | Stigmata of liver disease but no history of jaundice, ascites or bleeding oesophageal varices within the last five years and Liver function tests normal or mildly abnormal. |
15 | Episodes of biliary colic three to five times a year. |
20 | Stigmata of liver disease with jaundice, ascites or bleeding oesophageal varices one to five years ago and liver function tests now normal or mildly abnormal. |
25 | Stigmata of liver disease with jaundice, ascites or bleeding oesophageal varices one to five years ago and liver function tests markedly abnormal. |
40 | Stigmata of liver disease with jaundice, ascites or bleeding oesophageal varices in the past year or objective signs of progressive liver disease. |
50 | Permanent irreparable biliary tract obstruction. |
60 | Objective signs of progressive liver disease with one of the following: - persistent jaundice
- frequent, recurrent bleeding episodes
- central nervous system manifestations of hepatic insufficiency.
|
70 | Objective signs of progressive liver disease with two of the following: - persistent jaundice
- frequent, recurrent bleeding episodes
- central nervous system manifestations of hepatic insufficiency.
|
80 | Objective signs of progressive liver disease with all of the following: - persistent jaundice
- frequent, recurrent bleeding episodes
- central nervous system manifestations of hepatic insufficiency.
|
95 | Hepatic coma. |
% WPI | Description of level of impairment |
5 | Any of the following: - inguinal hernia (readily reducible)
- ventral hernia, well supported.
|
10 | Any of the following: - small recurrent inguinal hernia (operable but not readily reducible)
- colostomy.
|
15 | Any of the following: - large recurrent inguinal hernia (inoperable and not readily reducible)
- oesophagostomy
- gastrostomy
- ventral hernia, not well supported.
|
20 | Any of the following: - massive ventral hernia (inoperable, with severe diastasis of recti)
- jejunostomy
- ileostomy.
|
Introduction
These tables are intended to be used to assess impairment arising from specific joint lesions or amputations.
Where the joints function normally but the use of a limb is restricted for other reasons, for example soft tissue injury, nerve injury or bony injury not involving joints, Table 9.4 (Limb function—upper limb) or 9.5 (Limb function—lower limb) should be used.
These Tables can be used to assess the impairment of overall limb function from any cause.
Notes
- Either the musculo-skeletal table or Table 9.4 or 9.5 should be used—not both.
- Assessment is in accordance with the range of joint movement.
- X-rays should not be taken solely for assessment purposes.
Values are for one joint only. Where more than one joint is affected, values should be combined using Table 14.1 (Combined values chart).
% WPI | Description of level of impairment |
0 | X-ray changes but no loss of function of shoulder, elbow or wrist. |
5 | Any one of the following: - x-ray changes with minimal loss of function of shoulder, elbow or wrist
- ankylosis of any joint of ring and/or small finger(s).
|
10 | Any of the following: - loss of less than half normal range of movement of shoulder or elbow
- loss of half normal range of movement of wrist
- ankylosis of any joints of index and/or middle finger(s).
|
15 | Any of the following: - loss of more than half normal range of movement of wrist
- ankylosis of any joint(s) of thumb.
|
20 | Any of the following: - loss of half normal range of movement of shoulder or elbow
- ankylosis of wrist.
|
30 | Loss of more than half normal range of movement of shoulder or elbow |
40 | Ankylosis of shoulder or elbow. |
Assessment is in accordance with the range of joint movement. X-rays should not be taken solely for assessment purposes.
Where a joint has been surgically replaced assessment is in accordance with its function.
Shortening of the lower extremity by 2.5cm or more is an impairment of 5%.
For conditions not covered (such as flail joints) the assessor should have regard to the loss of function (not exceeding the maximum allowed for amputation).
Values are for one joint only. Where more than one joint is affected, values should be combined using Table 14.1 (Combined values chart).
% WPI | Description of level of impairment |
0 | X-ray changes but no loss of function of hip, knee or ankle or ankylosis or lesser changes in any toes except the hallux. |
5 | Loss of less than half normal range of movement of ankle. |
10 | Any of the following: - loss of less than half normal range of movement of hip or knee
- loss of half normal range of movement of ankle
- ankylosis of hallux.
|
15 | Loss of more than half normal range of movement of ankle. |
20 | Any of the following: - loss of half normal range of movement of hip or knee
- ankylosis of ankle.
|
30 | Loss of more than half normal range of movement of hip or knee. |
40 | Ankylosis of hip or knee. |
Impairment relating to the loss of or injury to a finger or toe refers not only to amputation or total loss of efficient use of the whole digit, but also to partial loss of efficient use of a digit.
% WPI | Description of level of impairment |
5 | Any of the following: - amputation of little finger
- amputation of ring finger
- total loss of movement of any joint of thumb
- amputation of terminal segment of thumb involving one third of its flexor surface without loss of distal phalanx or interphalangeal joint
- amputation of two phalanges or joints of index, middle, ring or little finger
- amputation of distal phalanx or joint of forefinger
- amputation of distal phalanx or joint of hallux.
|
10 | Any of the following: - amputation of all toes
- amputation of great toe
- amputation of middle finger
- amputation of distal phalanx or joint of thumb.
|
15 | Any of the following: - mid-metatarsal amputation
- amputation of index finger.
|
20 | Any of the following: - partial amputation of the foot (Chopart)
- amputation of the thumb.
|
30 | Any of the following: - amputation below knee, with functional stump
- amputation at ankle
- amputation of all fingers, but not thumb.
|
40 | Any of the following: - amputation above knee with functional stump
- disarticulation at knee
- Gritti Stokes amputation
- amputation below knee with short stump (7.5 cm or less below intercondylar notch)
- disarticulation at hip joint
- amputation above knee with short stump (7.5 cm or less below tuber ischii).
|
50 | Any of the following: - hemipelvectomy
- amputation of forearm distal to biceps tendon insertion
- disarticulation at wrist joint
- mid-carpal or mid-metacarpal amputation of hand.
|
60 | Any of the following: - amputation between deltoid insertion and elbow
- disarticulation at elbow
- amputation of forearm proximal to biceps tendon insertion
- disarticulation at shoulder
- amputation above deltoid insertion.
|
70 | Forequarter (upper) amputation. |
% WPI | Description of level of impairment |
10 | Can use limb for self-care and grasping and holding but has difficulty with digital dexterity. |
20 | Can use limb for self-care but has no digital dexterity or has difficulties grasping and holding. |
30 | Retains some use of limb but has difficulty with self-care. |
40 | Cannot use limb for self-care. |
% WPI | Description of level of impairment |
10 | Can rise to standing position and walk but has difficulty with grades and steps. |
20 | Can rise to standing position and walk but has difficulty with grades, steps and distances. |
30 | Can rise to standing position and walk with difficulty but is limited to level surfaces. |
50 | Can rise to standing position and maintain it with difficulty but cannot walk. |
65 | Cannot stand or walk. |
Lesions of the sacrum and coccyx should be assessed by using the table which most appropriately reflects the functional impairment. This will usually be Table 9.5 (Limb function—lower limb).
Lesions of the spine are often accompanied by neurological consequences. These should be assessed using Table 9.4 (Limb function—upper limb) or 9.5 (Limb function—lower limb) and the results combined using Table 14.1 (Combined values chart).
% WPI | Description of level of impairment |
Cervical spine | Thoraco-lumbar spine |
0 | X-ray changes only. | X-ray changes only. |
5 | Minor restrictions of movement. | Minor restrictions of movement or crush fracture - compression of 25% to 50%. |
10 | Loss of half normal range of movement. | Loss of less than half normal range of movement or crush fracture—compression greater than 50%. |
15 | Loss of more than half normal range of movement. | Loss of half normal range of movement. |
20 | Complete loss of movement. | Loss of more than half normal range of movement. |
30 | | Complete loss of movement. |
% WPI | Description of level of impairment |
0 | Diminution of upper urinary tract function is present as evidenced by creatinine clearance of 90 litres/day or more and/or intermittent symptoms or signs of upper urinary tract dysfunction are present that do not require continuous treatment or surveillance. |
10 | Diminution of upper urinary tract function is present as evidenced by creatinine clearance of 75 to 89 litres/day and/or single kidney. |
15 | Creatinine clearance is 75 to 89 litres/day AND symptoms and signs of urinary tract dysfunction or disease necessitate continuous medical treatment. |
30 | Diminution of upper urinary tract function is present as evidenced by creatinine clearance of 60 to 74 litres/day. |
40 | Diminution of upper urinary tract function is present as evidenced by creatinine clearance of 50 to 59 litres/day. |
45 | Diminution of upper urinary tract function is present as evidenced by creatinine clearance of 50 to 59 litres/day and symptoms and signs of dysfunction or disease are incompletely controlled by surgical or continuous medical treatment. |
60 | Diminution of upper urinary tract function is present as evidenced by creatinine clearance of 40 to 49 litres/day. |
65 | Diminution of upper urinary tract function is present as evidenced by creatinine clearance of 40 to 49 litres/day and symptoms and signs of dysfunction or disease are incompletely controlled by surgical or continuous medical treatment. |
70 | Diminution of upper urinary tract function is present as evidenced by creatinine clearance of less than 40 litres/day. |
75 | Diminution of upper urinary tract function is present as evidenced by creatinine clearance of less than 40 litres/day and symptoms and signs of dysfunction or disease are incompletely controlled by surgical or continuous medical treatment. |
85 | Deterioration of renal function requiring either peritoneal dialysis or haemodialysis. |
% WPI | Description of level of impairment |
0 | Occasional intermittent disorder without interval problems. |
10 | Uretheral stricture or other disorder requiring intermittent therapy (for example, passage of sounds at intervals of greater than eight weeks). |
15 | Disorder requires continuous treatment or no voluntary bladder control but good reflex activity. |
25 | Urinary diversion with or without removal of the bladder or uretheral stricture or other disorder which cannot be effectively controlled, or recurs frequently, or requires more frequent passage of sounds (at intervals of less than four to eight weeks). |
30 | Intermittent dribbling incontinence. |
45 | Continuous dribbling incontinence. |
This table is used to assess conditions affecting the testes, prostate, penis, seminal vesicles, spermatic cord, epididymis and scrotum.
% WPI | Description of the level of impairment |
5 | Any of the following: - only one testis present
- symptoms and/or signs of scrotal loss or disease
- scrotal malposition
or all of the following: - symptoms and/or signs of testicular, epididymal and/or spermatic cord disease, WITH anatomical alteration
- continuous treatment not required
- no seminal or hormonal abnormalities
or all of the following: - symptoms and/or signs of prostatic and/or seminal vesicular dysfunction or disease
- anatomical alteration present
- continuous treatment not required
or - impotence in a claimant aged 65 years or more with intact sexual organs.
|
10 | Sexual function possible but varying degrees of difficulty with erection, ejaculation and/or sensation. |
15 | Any of the following: - sexual function possible in that there is sufficient erection but no ejaculation or sensation
- testes implanted in other than scrotal position to preserve function and testicular pain or discomfort with activity
- total loss of scrotum
- impotence in a claimant aged between 40 and 64 years with intact sexual organs
or all of the following: - symptoms and/or signs of testicular, epididymal and/or spermatic cord disease, with anatomical alteration
- continuous or frequent treatment required
- detectable seminal or hormonal abnormalities
or all of the following: - frequent severe symptoms and/or signs of prostatic and/or seminal vesicular function or disease
- anatomical alteration present
- continuous treatment required.
|
20 | No sexual function possible because of any of the following: - bilateral loss of testes
- no detectable seminal or hormonal function of the testes, epididymis or spermatic cords
- ablation of prostate and/or seminal vesicles
or - impotence in a claimant aged less than 40 years with intact sexual organs.
|
% WPI | Vulva and/or vagina | Cervix and/or uterus | Fallopian tubes and/or ovaries |
10 | Symptoms and/or signs of disease or deformity not requiring continuous treatment and sexual intercourse possible and vagina adequate for childbirth. | Symptoms and/or signs of disease or deformity not requiring continuous treatment or cervical stenosis not requiring treatment or anatomical loss in post- menopausal years. | Symptoms and/or signs of disease or deformity not requiring continuous treatment or unilateral dysfunction or bilateral loss in post- menopausal years. |
25 | Symptoms and/or signs of disease or deformity requiring continuous treatment and sexual intercourse possible with varying degrees of difficulty and vaginal delivery limited in pre-menopausal years. | Symptoms and/or signs of disease or deformity requiring continuous treatment or cervical stenosis requiring periodic treatment. | Symptoms and/or signs of disease or deformity requiring continuous treatment but tubes are patent and ovulation is possible. |
35 | Symptoms and/or signs of disease or deformity not controlled by continuous treatment and sexual intercourse not possible and vaginal delivery not possible in the pre-menopausal years. | Symptoms and/or signs of disease or deformity not controlled by continuous treatment or cervical stenosis complete or anatomical or complete functional loss in the pre-menopausal years. | Symptoms and/or signs of disease or deformity not controlled by continuous treatment and total loss of tubular patency, or total failure to produce ova, in the pre-menopausal years. |
% WPI | Description of level of impairment |
10 | Any of the following. - female of childbearing age with absence of the breasts
- male with painful gynaecomastia that interferes with daily activities
- galactorrhoea sufficient to require the use of absorbent pads.
|
Introduction
Neurological function is divided into three sub-groups—cranial nerves (Table 12.1), communication (Tables 12.2 & 12.3) and cognitive function (Tables 12.4 & 12.5).
Communication and cognitive function are each divided into two sub-sections—the sub-sections of communication are comprehension (Table 12.2) and expression (Table 12.3); the sub-sections of cognitive function are memory (Table 12.4) and reasoning (Table 12.5).
Tables 12.2 to 12.5 should not be used to assess problems whose origins are genetic, social or educational. Their use is confined to the assessment of the consequences of neurological injury or disease.
Please note that assessments for sight, smell and taste can be made under other tables. They have been included here as well so that this table is complete.
Do not make two separate assessments and combine them. Use one or the other.
The other relevant tables are Table 6.1 (Disorders of visual acuity), and Table 7.2 (Miscellaneous ear, nose and throat disorders).
% WPI | Criteria |
Unilateral loss or paralysis | Bilateral loss or paralysis | Other |
0 | I
XII | I | |
5 | V (motor) | VII (complete loss of taste). | |
10 | V (sensory) | XII (swallowing impairment, with diet restricted to semi-solids). | Swallowing impairment due to one or two combinations of IX, X and XI, with diet restricted to semi- solids. |
15 | VII | | |
20 | | | VII Atypical facial neuralgia. |
25 | II or III, IV, VI alone or in combination (diplopia corrected by covering one eye). | | |
30 | | XII (swallowing impairment, with diet restricted to liquids). | Swallowing impairment due to one or two combinations of IX, X and XI, with diet restricted to liquids. |
35 | | V (sensory) | |
45 | | V (motor) | |
50 | | | V Intractable typical trigeminal neuralgia or tic douloureux. |
60 | | XII (swallowing impairment, with diet by tube feeding or gastrostomy). | Swallowing impairment due to one or two combinations of IX, X & XI, and resulting in diet by tube feeding or gastrostomy. |
85 | | II | |
Communication
- Communication disorders may arise as a result of interference with comprehension and/or expression. They are the result of neurological damage arising, for example, from head injury or cerebro-vascular accident.
- Comprehension may be further divided into hearing and reading skills, and expression into verbal and written skills. A report from a Speech Pathologist or Rehabilitation Specialist will generally be necessary to enable impairment of this function to be accurately assessed.
- In all cases the employee’s abilities prior to the injury or disease must be taken into account. It would be inappropriate to assess an illiterate person with respect to reading and writing skills. Similarly where English is an employee’s second language, it may be more appropriate to base assessment on interference with ability to understand and speak the employee’s first language.
% WPI | Criteria |
Hearing (see note below) | Reading |
5 | Understands speech in most situations, but has difficulties in groups or when fatigued. | Reads books and magazine articles, but does not understand details. |
10 | Understands speech in one-to-one situations, but cannot cope in group situations. | Can get the gist of simple articles, for example in newspapers, but has great difficulty with details. |
20 | | Understands only simple sentences. |
25 | Understands simple sentences although repetition is sometimes needed. | |
30 | | Able to read only single words. |
35 | | Unable to read at all. |
40 | Able to understand only single words. | |
50 | Unable to understand any language. | |
Note
- Hearing refers to the ability to comprehend spoken language—that is, with the ability to interpret auditory signals, not to receive such signals. It does not refer to hearing impairment, which is assessed using Table 7.1 (Hearing).
% WPI | Criteria |
Verbal | Written |
5 | Can sustain conversation, but has minor word retrieval problems and/or hesitancy. | Can write simple letters, but cannot write complex documents. |
10 | Can converse in simple sentences only and may have difficulty with word finding and expressing complex ideas. | Can write postcards and letters of about five lines (spelling and grammatical errors may be apparent), but cannot write longer documents. |
15 | | Can write only short, simple sentences (spelling errors may be evident). |
20 | Only able to respond in short sentences or phrases. | Cannot write sentences, but can write single words. |
25 | | Able to write or copy only a familiar sequence of letters, for example own name or unable to write at all. |
30 | Limited to use of single words and/or social or stereotyped phrases. | |
35 | No useful speech (includes unintelligible speech and speech limited to swearing). | |
% WPI | Criteria |
0 | No appreciable effect. Reliance on notes, lists etc is comparable to others of same age, education and lifestyle. |
10 | Difficulties with names and appointments and tends to misplace objects. There may be partial compensation by reliance on notes, lists, diaries or other people. |
25 | Failure to keep appointments or fulfil other obligations despite use of memory aids and difficulties recalling details of recent events AND tendency to get lost in unfamiliar surroundings. |
40 | Failure to keep appointments or fulfil other obligations despite use of memory aids, to a more pronounced extent and some supervision by another necessary. |
60 | Unable to recall recent events or experiences and constant supervision necessary to avoid harm, resulting in inability to live independently. |
70 | Unable to recall recent events or experiences, to a more pronounced extent and disorientation in familiar surroundings and inability to recognise familiar faces or objects. |
Notes
- Cognitive function has two components—memory and reasoning ability. These functions are affected where there is neurological damage, for example from head injury, cerebro-vascular accident etc.
- Difficulties with memory or reasoning ability due to some other process, for example psychiatric illness, should not be assessed using these tables. Instead Table 5.1 (Psychiatric conditions) should be used.
- Assessment should be carried out by a neurologist or clinical psychologist.
% WPI | Criteria |
0 | Abilities intact. |
10 | Able to cope with routine activities and situations but experiences minor difficulties in new situations. |
25 | Still able to cope with routine activities but has moderate difficulties in new
situations and complex decision-making and abstract thinking are affected. |
40 | Major difficulties in new situations and difficulties with routine activities and problems becoming manifest and complex decision-making and abstract thinking seriously affected. |
60 | Major difficulties in carrying out routine daily activities. Perseverative thinking may be evident. |
70 | Needs prompting and assistance with even the simplest activities. |
Notes
- Assessment is carried out by examining the degree of interference with the ability to plan and carry out tasks involving a number of steps, ability to solve problems and make decisions which involve the examination of new and old material, and the ability to think in abstract terms: for example, to interpret proverbs. Generally complex tasks and decisions will be first affected as will decisions involving unfamiliar factors.
- Assessment should be carried out by a neurologist or clinical psychologist.
For use in the assessment of disorders of the haemopoietic system such as anaemia, polycythaemia, leucocyte and platelet disorders and intermittent disorders such as asthma, migraine, tension headache, epilepsy etc.
Principles
Determine the frequency, duration and severity of attacks with reference to the degree of interference with activities of daily living.
% WPI | Description of level of impairment |
0 | Episodes may be of any frequency but do not interfere with activities of daily living
or are readily prevented or reversed by appropriate medication or treatment. |
10 | Episodes occur 12 or more times a year and cause minor interference with activities of daily living or episodes occur less frequently and cause interference with all activities of daily living other than self-care. |
20 | Episodes occur up to 25% of the time and cause significant interference with most activities of daily living other than self-care. |
30 | Episodes occur up to 30% of the time and cause significant interference with most activities of daily living other than self-care. |
40 | Episodes occur up to 40% of the time and cause significant interference with most activities of daily living other than self-care. |
50 | Episodes occur up to 50% of the time and cause significant interference with most activities of daily living other than self-care. |
60 | Episodes occur up to 60% of the time and cause significant interference with most activities of daily living other than self-care. |
70 | Episodes occur up to 70% of the time and cause significant interference with most activities of daily living other than self-care. |
75-95 | Episodes occur 75% to 100% of the time and needs assistance with most or all activities of daily living including self-care (confinement to a residential care facility is required for assessed impairment levels of more than 80%). |
Note
% WPI | Description of level of impairment |
0 | No symptoms or evidence of disease and able to undertake normal activities with no special care needed. |
10-15 | Some signs or symptoms of disease and normal activities can be undertaken with moderate effort. |
35 | Does not require institutional care but needs assistance with activities of daily living other than self-care. |
50 | Can still be maintained at home but with considerable assistance and frequent medical care. |
65 | Requires institutional care and considerable assistance with activities of daily living other than self-care. |
75 | Requires institutional care and considerable assistance with activities of daily living including self-care. |
85 | Intensive support and/or treatment needed (disease may be progressing rapidly). |
Note
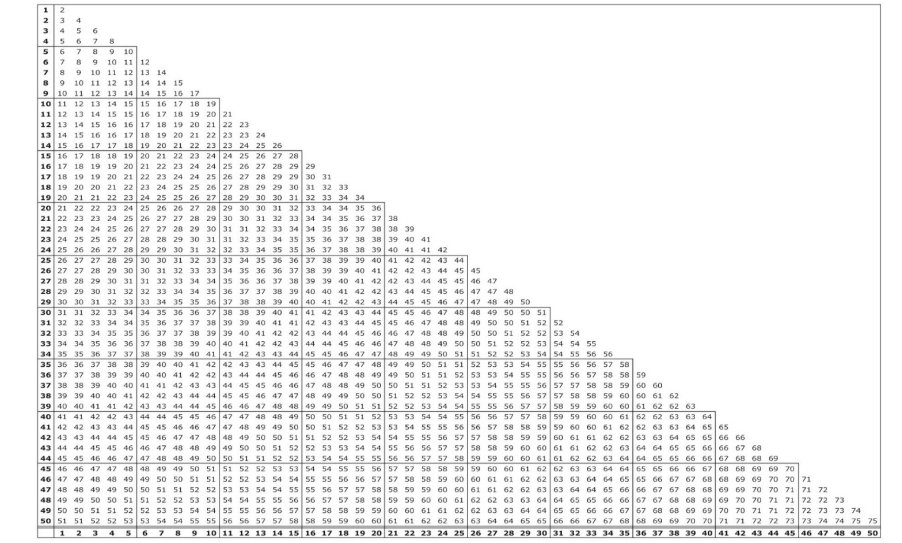
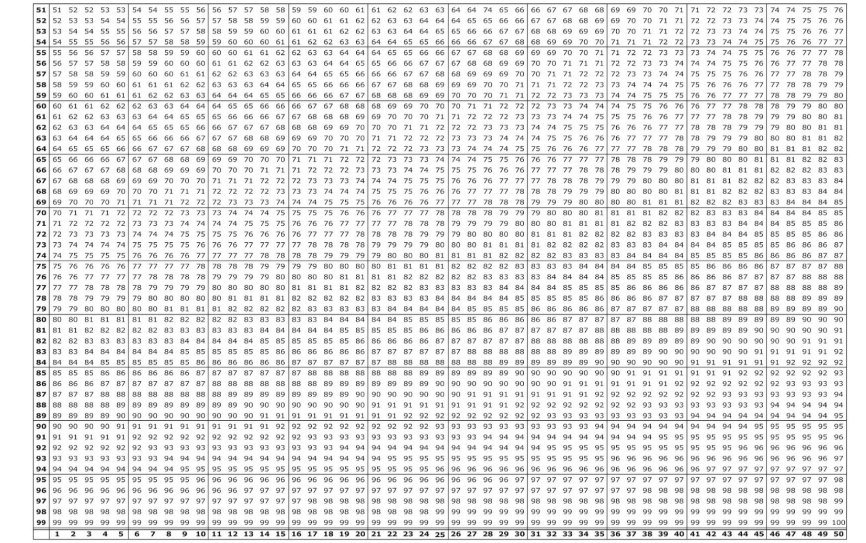
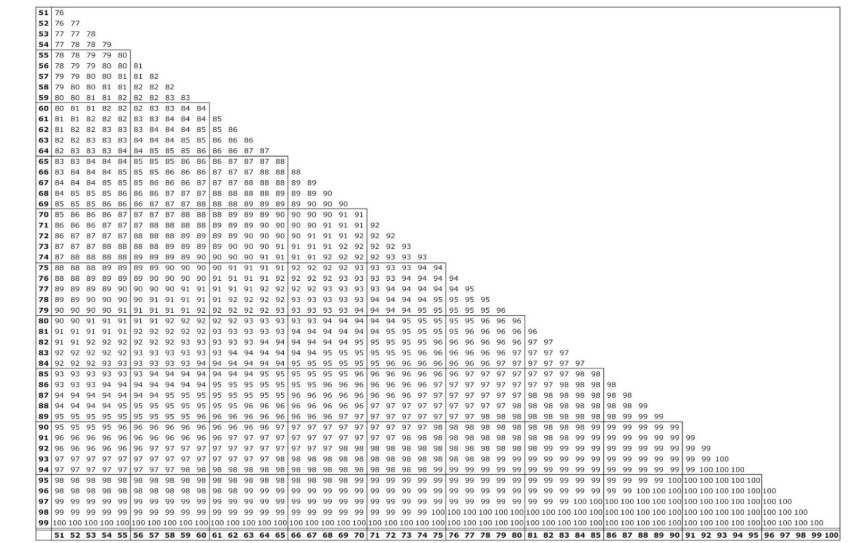
Introduction
The values are derived from the formula:
A + B(1-A) = combined value of A and B
where A and B are the decimal equivalents of the WPI ratings.
In the chart all values are expressed as percentages. To combine any two impairment values, locate the larger of the values on the side of the chart and read along that row until you come to the column indicated by the smaller value at the bottom of the chart. At the intersection of the row and the column is the combined value.
Example: To combine 35% and 20%, read down the side of the chart until you come to the larger value, 35%. Then read across the 35% row until you come to the column indicated by 20% at the bottom of the chart. At the intersection of the row and column is the number 48.
Therefore, 35% combined with 20% is 48%.
Because of the construction of this chart, the larger impairment value must be identified at the side of the chart.
If three or more impairment values are to be combined, sort the impairment values from highest to lowest, select the highest and second highest, then find their combined values as above. Then use that combined value and the third highest impairment value to locate the combined value of all impairments.
This process can be repeated indefinitely, the final value in each instance being the combination of all the previous values. In each step of this process the larger impairment value must be identified at the side of the chart.